FLOODS - Treatment in Lisbon
Specialised assessment and treatment for Episodic and Chronic Migraine in Lisbon - differential diagnosis, preventive therapy and neuromodulation with EMT
WHAT IS MIGRAINE?
Pain originating in the brain
Migraine is a chronic, recurring neurological disease characterised by episodes of moderate to severe headache - usually one-sided and pulsatile - accompanied by nausea, vomiting, photophobia (light) and phonophobia (sound). It is the 2nd leading cause of disability worldwide and the 1st in women between the ages of 15 and 49 - a clinical reality that requires specialised diagnosis and treatment.
Phases of the crisis and characteristic symptoms
- Prodrome - hours to days before the painMood swings, fatigue, frequent yawning, neck stiffness, and increased sensitivity to light or sound - early signs that precede the crisis and which, if identified, allow for more effective treatment.
- Aura - temporary neurological symptomsIt happens in around 30% of cases. It can cause visual changes, tingling or speech difficulties, which last between 20 and 60 minutes and disappear completely.
- Headache - the main phaseModerate to severe, unilateral (in 60% of cases), pulsating pain, lasting 4 to 72 hours, which leads the patient to seek a dark, quiet environment.
- Post-drome - the "migraine hangover"After the pain resolves, many patients experience intense fatigue, difficulty concentrating and a sense of cognitive emptiness, which can persist for 24 to 48 hours and also compromise their quality of life.
CLINICAL FORMS AND ASSOCIATED FACTORS
Migraine Without Aura - The Most Common Form
It accounts for around 70% of cases. Diagnosis is clinical and requires exclusion of secondary causes. Early abortive treatment and prevention are fundamental pillars.
Primary HeadacheMigraine With Aura - Focal Neurological Phenomena
Present in 30% of patients. Migraine with aura is associated with increased cardiovascular risk, especially in female smokers on oral contraception - which has direct therapeutic implications.
Higher CV riskChronic Migraine - 15 or More Days of Pain per Month
It is defined by the presence of headache on 15 or more days a month for more than 3 months, with migraine characteristics on at least 8 of those days. Often associated with symptomatic drug abuse. Requires powerful preventive therapy and, in refractory cases, anti-CGRP antibodies or botulinum toxin (botox).
Chronic migraineTriggering Factors and Genetic Predisposition
Migraine has a strong hereditary component - the risk is 3 to 4 times higher in first-degree relatives. The main triggers include sleep disturbances, stress, hormonal changes (menstruation, ovulation), fasting, alcohol, certain foods and intense sensory stimuli. Identifying and managing triggers is a central part of the therapeutic plan.
Genetics and Environment
Migraines are 3 times more common in women - fluctuating oestrogen levels are one of the main modulators of cortical excitability.
FLOODING: IMPACT, PREVALENCE
AND EFFECTIVENESS OF TREATMENT
The most disabling neurological disease in young adults - and one of the most underdiagnosed in Portugal
* Data based on published epidemiological studies and clinical trials. Individual results may vary.






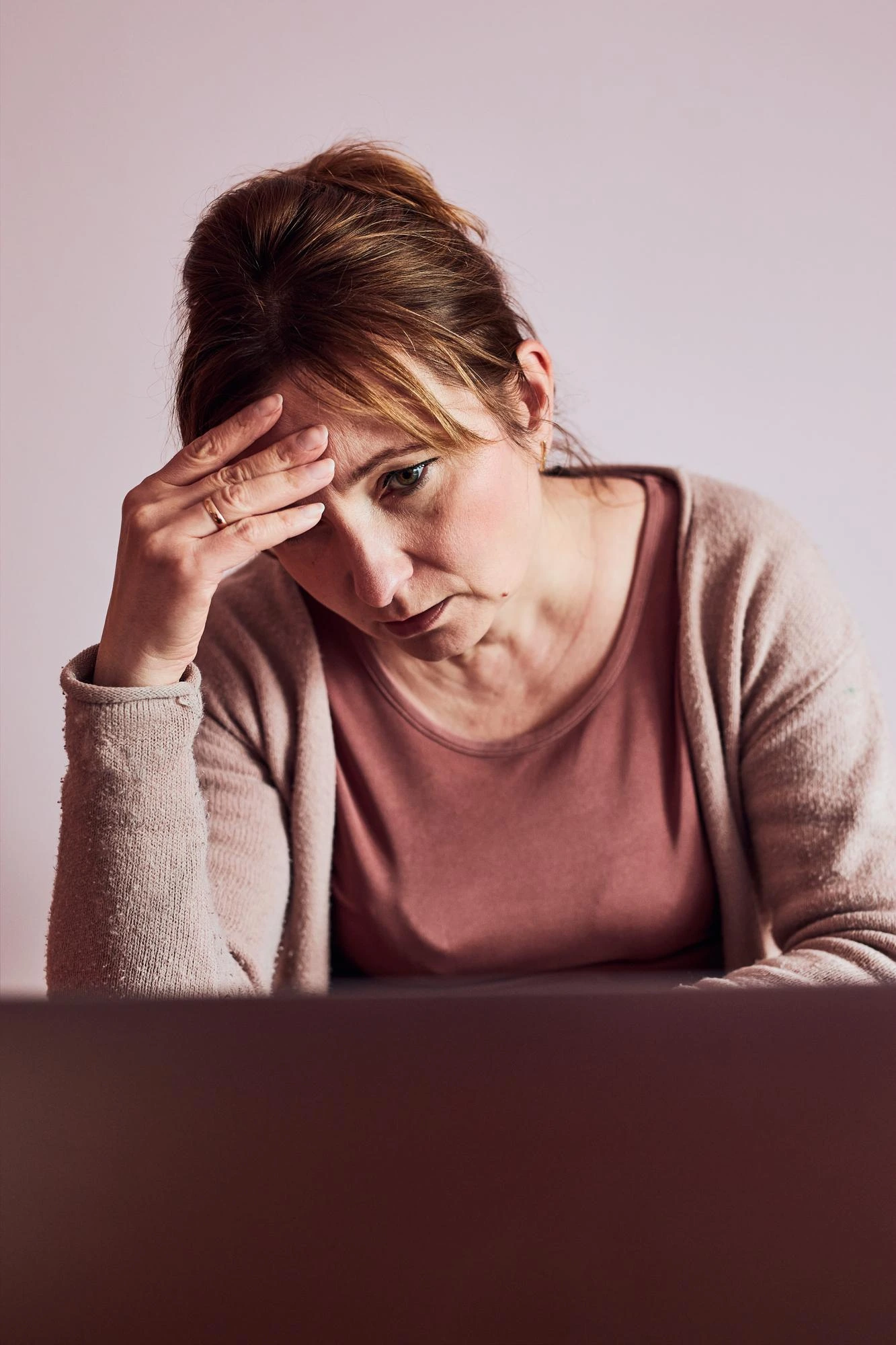
IMPORTANCE OF SPECIALISED CONSULTATION
Migraine can be extremely disabling. What's more, it is inadequately treated by the health system, with over-the-counter painkillers. This reality has direct consequences: without adequate preventive treatment, episodic migraine tends to become chronic, the frequency of attacks increases, and the growing use of symptomatic analgesics creates a cycle of dependence and aggravation - medication abuse headache - which overlaps and potentiates the underlying disease.
At NeuroPsyque, the Migraine consultation includes a structured neurological assessment with full characterisation of the pattern of crises, identification of triggering factors and chronification, assessment of the functional impact and quality of life, and preparation of an individualised therapeutic plan. We offer access to the entire therapeutic chain - from optimised abortive treatment to oral preventive therapy, to neuromodulation protocols with EMT - with continuous follow-up and adjustment according to clinical response.