RIGID MEN'S DISEASE - Treatment in Lisbon
Specialised assessment and treatment for Stiff Man Syndrome in Lisbon - diagnosis, treatment and follow-up
WHAT IS RIGID MAN'S DISEASE?
A rare and often underdiagnosed autoimmune disease
Stiff Man's Disease (SPS) is a rare autoimmune neurological disease characterised by progressive muscle rigidity, painful muscle spasms and great sensitivity to stimuli such as noise or touch. In most cases, it is related to antibodies (anti-GAD65) that affect a substance in the brain responsible for “calming” nerve activity, leading to over-excitement of the nerves.
Characteristic signs and symptoms
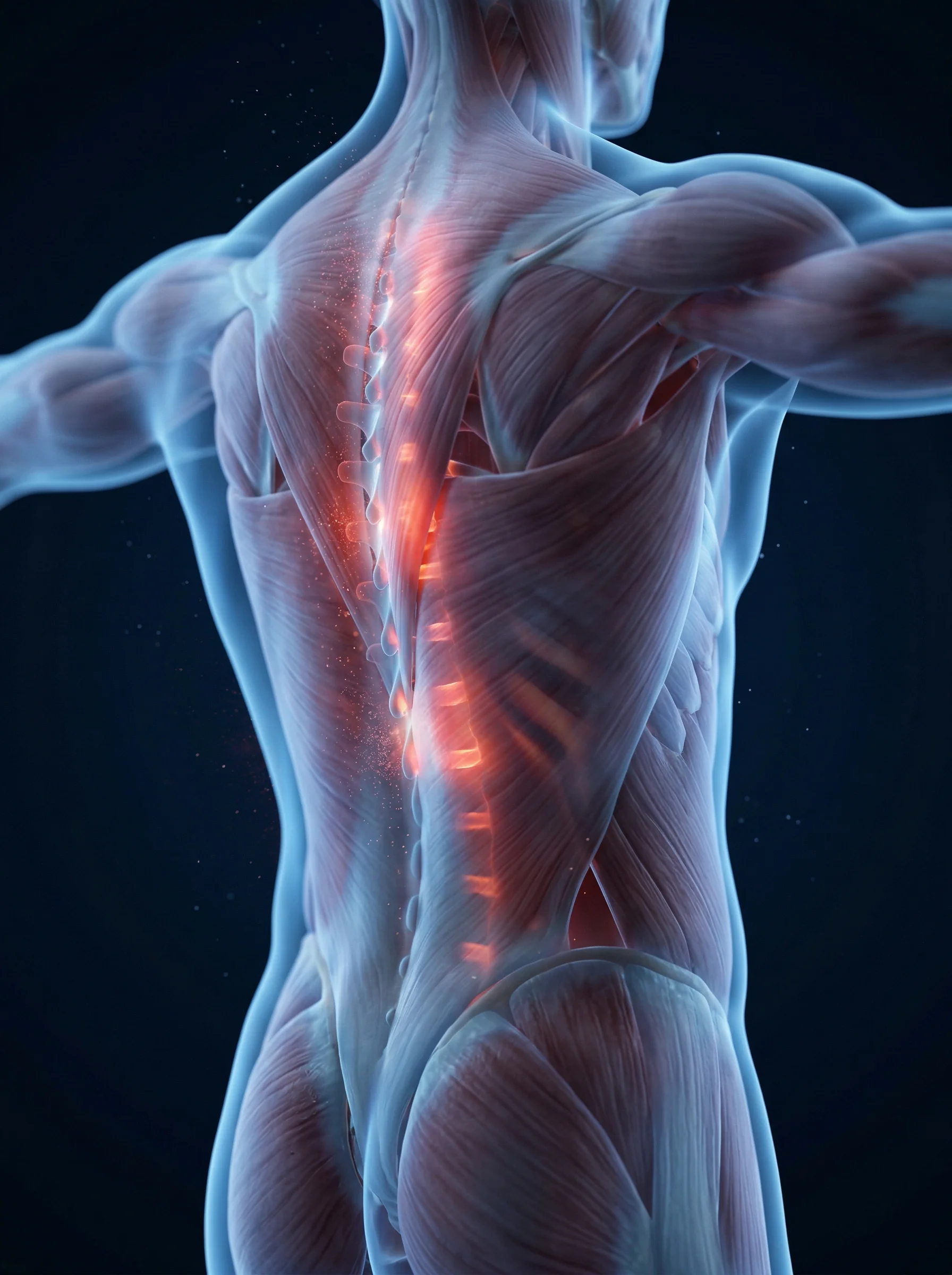
- Muscle stiffness in the trunkStrong, painful stiffness in the muscles of the back and abdomen, which can vary throughout the day and worsen with stress or stimuli such as noise or touch.
- Sudden, painful muscle spasmsViolent muscle contractions triggered by noise, unexpected touch, emotions or movement - with the risk of fractures and falls.
- Hypersensitivity to external stimuliExaggerated (involuntary) reactions to sound, tactile or visual stimuli that usually do not provoke a significant motor response.
- Anxiety, phobia and psychological disordersIntense anxiety, fear of leaving the house and fear of falling are common. These symptoms are not just a reaction to the disease - they are also linked to changes in the functioning of the nervous system.
VARIANTS, CAUSES AND CLINICAL ASSOCIATIONS
Classic SPS - Anti-GAD65 Antibodies
The most common form. It is associated with antibodies that interfere with the part of the nervous system responsible for reducing nerve activity. This leads to progressive body rigidity, spasms and increased muscle excitability. It can also be associated with other autoimmune diseases, such as type 1 diabetes and thyroid problems.
AutoimmuneParaneoplastic SPS - Anti-Amphiphysin and Others
It is associated with the presence of tumours, such as in the chest, lungs or thymus. The body produces antibodies that affect the nervous system. It is therefore essential to assess a possible oncological disease whenever this form is suspected.
ParaneoplasticStiff Limb Syndrome (SMS) - Focal Variant
This is a more localised form of the disease, in which the stiffness and spasms affect just one limb, usually one leg. It can make walking progressively more difficult and, in some cases, develop into a more generalised form.
FocalProgressive Encephalomyelitis with Rigidity (PERM)
This is a more serious form of the disease, which affects important areas of the nervous system. It can cause involuntary movements, difficulty swallowing, changes in eye movements and problems with automatic body control (such as heartbeat or blood pressure). It is associated with certain antibodies and generally requires more intensive treatment.
Severe variant
SPS is 2 to 3 times more common in women than in men, and is associated with other autoimmune diseases in more than 60% of cases - type 1 diabetes, thyroiditis, vitiligo and pernicious anaemia, among others.
SPS: DIAGNOSIS AND RESPONSE
IMMUNOTHERAPY
A rare disease with effective treatment - early diagnosis is decisive for prognosis
* Data based on published clinical studies and case series. Individual results may vary.
Sources: clinical data, NIH/PubMed - IGIV systematic review in Stiff-Person Syndrome (12 studies, 216 patients; 83,16% symptomatic improvement); Neurology.org - IGIV in GAD+ SPS: 67% significant improvement (36 patients, 40 months follow-up); NIH/PubMed - prevalence of anti-GAD65 in classic SPS (60-80%); NIH/PubMed - autoimmune comorbidities in SPS: type 1 diabetes in 35%, autoimmune thyroiditis in 38%.






IMPORTANCE OF SPECIALISED CONSULTATION
Stiff Man's Disease is one of the neurological diseases with the longest diagnostic delay - an average of 7 years from the first symptoms. The fluctuating stiffness (with variations over time) and painful spasms are often attributed to musculoskeletal problems, fibromyalgia or anxiety, and in some cases even to Parkinson's disease, which delays the correct diagnosis and the start of immunotherapy. This delay has direct consequences: the longer the disease goes untreated, the greater the risk of progression and serious complications such as falls, fractures and respiratory problems.
At NeuroPsyque, the Stiff Man's Disease consultation includes a structured neurological assessment, coordination of a complete serological study (anti-GAD65, anti-amphiphysin, anti-DPPX, anti-GlyR), research into occult neoplasia when indicated, and access to non-invasive neuromodulation protocols with EMT to control cortical hyperexcitability and symptomatic relief. Anxiety and phobia management and integrated psychological support are indispensable dimensions of our care model.