In Portugal, it is estimated that 18-20 thousand people live with Parkinson's disease - approximately 180 cases per 100,000 inhabitants. With the ageing of the Portuguese population, this figure could reach 30 thousand cases over the next two decades.
It's waking up in the morning and realising that your body no longer obeys as before. It's trying to button a shirt and finding that your fingers refuse to co-operate, moving with a frustrating slowness that didn't exist a few months ago. It's noticing that your handwriting, once firm and legible, has become progressively smaller and shakier. It's feeling the stiff muscles as if they were made of wood, especially in the morning, when every movement requires a conscious effort that should be automatic.
For those living with Parkinson's, it's not just "walking slower" or "shaking a bit". It's a complete reorganisation of the way the body moves through the worldThis is where simple actions such as getting up from a chair or turning round in bed become challenges that require planning and determination.
What is Parkinson's Disease?
Parkinson's disease is a progressive neurodegenerative condition which mainly affects the nervous system, resulting in the degeneration of neurons specialised in producing dopamine. This neurotransmitter is essential for movement control, coordination and various non-motor functions.
First described in 1817 by the English physician James Parkinson as "agitating paralysis"Today, this condition is recognised as one of the most complex neurological diseasesThis is characterised by much more than the tremors initially observed.
Medical Definition
According to International Classification of Diseases (ICD-11), Parkinson's is defined as a primary parkinsonian syndrome characterised by bradykinesia (slowness of movement) combined with resting tremor and/or muscle rigidity.
The condition results from the progressive loss of dopaminergic neurons - dopamine producers. Dopamine is a brain signal responsible for communication with the whole body.
Recognition in Portugal
In Portugal, Parkinson's disease is officially recognised as chronic disabling condition. The central hospitals register more than 1,800 new cases each year, with the speciality of movement disorders of the Coimbra Hospital and University Centre carries out around 2,600 consultations a year.
Difference between Parkinson's and other Movement Conditions
It is essential to distinguish Parkinson's disease from other conditions that can cause similar symptoms, especially Essential Tremor and normal ageing changes.
| Features | Parkinson's | Essential Tremor |
| Type of tremor | At rest, decreases with movement | During movement/action |
| Rigidity | Present: cogwheel (explanation below) | Absent |
| Slowness | Marked bradykinesia | Absent |
| Response to levodopa | Positive | Nil |
| Progression | Progressive and asymmetrical | Slow, symmetrical |
| Other symptoms | Non-motor symptoms | Rare |
| Features | Parkinson's | Age increase |
| Type of tremor | At rest, decreases with movement | Absent or minimal |
| Rigidity | Present: cogwheel (explanation below) | Lightweight, symmetrical |
| Slowness | Marked bradykinesia | Slight slowdown |
| Response to levodopa | Positive | Nil |
| Progression | Progressive and asymmetrical | Stable |
| Other symptoms | Non-motor symptoms | Age-related |
Essential Tremor affects approximately 1% of the population and is often confused with Parkinson's. However, in Essential Tremor, the tremor occurs during action (such as drinking water), while in Parkinson's is more evident at rest.

Most common symptoms of Parkinson's Disease
Parkinson's disease manifests itself through a wide range of symptoms that go far beyond the tremors traditionally associated with the condition.
Motor Symptoms
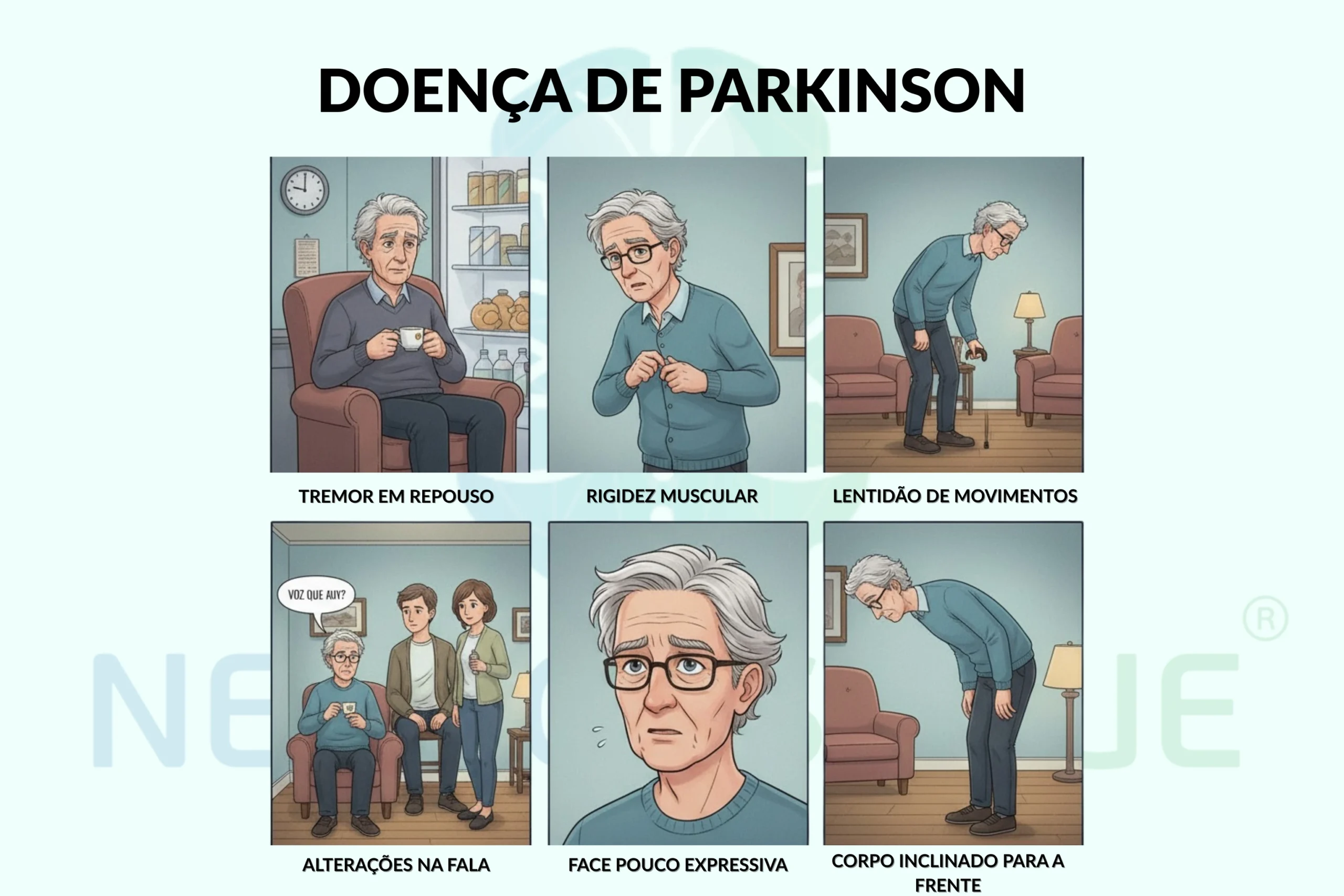
Motor symptoms form the core of Parkinson's disease and include:
Bradykinesia (slowness of movement)
Bradykinesia is considered the cardinal symptom of Parkinson's. It is characterised by generalised slowness of voluntary movements and a decrease in their amplitude. It manifests itself as difficulty initiating movements, a reduction in automatic movements (such as swinging the arms when walking) and early fatigue during repetitive activities.
Resting Tremor
Present in around 70-80% of patients, the resting tremor is typically unilateral at first, often starting in one hand. It has a frequency of 4-6 Hz and is described as "counting coins". Paradoxically, decreases or disappears during voluntary movement and worsens in situations of stress or anxiety.
Muscle stiffness
Rigidity in Parkinson's is characterised by an increase in the muscle tension that persists regardless of the speed of passive movement. When combined with tremor, it produces the phenomenon of "cogwheel". This symptom is characterised by a feeling of intermittent resistance during movement - like a rusty sprocketinstead of running smoothly and fluidly, it progresses by leaps and bounds. bumpsThere are times when movement is almost non-existent.
Postural instability
It usually appears in more advanced stages of the disease, manifesting as difficulty maintaining balance, tendency to fall and changes in gait. Patients develop a stooped posture and walk in small, dragging steps.
Non-motor symptoms
Non-motor symptoms are prone to, and are often underdiagnosedBut they can be just as incapacitating as motorised ones:
Sleep Changes
- REM sleep behaviour disorder (acting during dreams)
- Insomnia and fragmented sleep
- Excessive daytime sleepiness
- Restless legs syndrome
Cognitive and Psychiatric Changes
- Mild cognitive impairment (in 15-20% of initial cases)
- Depression (affects 40% patients)
- Anxiety and panic attacks
- Apathy and loss of motivation
- Visual hallucinations (in advanced stages)
Autonomic dysfunctions
- Orthostatic hypotension
- Chronic constipation
- Urinary dysfunction
- Sexual dysfunction
- Changes in thermal regulation
Sensory changes
- Hyposmia (reduced sense of smell) - can precede motor symptoms by years
- Pain and paresthesia
- Central pain syndrome
Types and Stages of Parkinson's
Classification by Symptom Predominance
Dominant Tremor Subtype
- Prominent tremor with slower progression
- Better cognitive prognosis
- Good initial response to dopaminergic medication
Postural Instability/Gait Difficulty Subtype (PIGD)
- Predominance of rigidity and bradykinesia
- Increased risk of cognitive decline
- Less predictable response to levodopa
Mixed Subtype
- Balanced combination of symptoms
- Intermediate progression
Classification by Starting Age
Young onset Parkinson's (before the age of 50)
- Represents 5-10% of cases
- Greater genetic component
- Slower progression initially
- Increased risk of early dyskinesias with levodopa
Late Onset Parkinson's (after 65 years)
- Potentially faster progression
- Increased risk of cognitive decline
- Better initial tolerance to levodopa

Causes and risk factors
Parkinson's disease results from a complex interaction between genetic predisposition and environmental factorsThere is no single identifiable cause.
Genetic factors
Approximately 10-15% of cases have a clear family component. More than 20 genetic variants associated with Parkinson's, that can be testedThe most important of these are:
- LRRK2 (particularly prevalent in Portugal)
- PARK2 (parkina)
- PINK1
- DJ1
- SNCA (α-synuclein)
Environmental factors
- Exposure to pesticides and herbicides: Increases the risk in 70%
- Heavy metals: Manganese, iron, copper
- Head trauma: Especially repetitive
- Viral infections: Encephalitis, influenza
- Industrial solvents: TCE, PCE
Demographic Risk Factors
- Age: Main risk factor (incidence doubles every decade after 60)
- Sex: Men have a 1.5-2x higher risk
- Ethnicity: Higher prevalence in Caucasians
Protective Factors
- Coffee consumption (risk reduction up to 60%)
- Smoking (paradoxically protective, but not recommended)
- Regular physical exercise
- Mediterranean diet
- Moderate alcohol consumption
The Diagnosis of Parkinson's Disease
The diagnosis of Parkinson's disease is based on fundamentally in clinical assessmentThere is currently no definitive diagnostic test.
Diagnostic Criteria
A Movement Disorder Society established updated diagnostic criteria that include:
Absolute Criteria
- Bradykinesia combined with at least one of the following:
- Resting tremor (4-6 Hz)
- Muscle stiffness
Support Criteria
- Unilateral onset and persistent asymmetry
- Positive response to dopaminergic therapy (levodopa)
- Presence of levodopa-induced dyskinesias (involuntary muscle movements)
- Hyposmia (impaired sense of smell) or low blood pressure
Red Flags
- Rapid development (wheelchair in 5 years)
- Complete lack of response to levodopa (dopamine replacement drug)
- Early ataxia (loss of coordination)
- Early postural instability
- Difficulty swallowing and early speech problems
- Hallucinations not related to medication
Diagnostic Process
- Detailed clinical history: Time course of symptoms, response to medication, family history
- Neurological examination: Assessment of cardinal signs, gait, postural reflexes
- Therapeutic test: Response to levodopa (improvement ≥30% in the UPDRS - Unified Parkinson's Disease Rating Scale)
- Complementary tests: Only to the exclusion of other causes
- DaTscan: In doubtful cases (shows reduced uptake in the basal ganglia)
Impact of Parkinson's on daily life
Parkinson's profoundly affects multiple dimensions of lifeThe impact extends far beyond the visible motor symptoms.
Physical and Functional Impact
- Progressive reduction in capacity for activities of daily living
- Difficulties with personal hygiene, food and clothing
- Changes in gait with a greatly increased risk of falls (30-60% of patients)
- Deteriorating sleep quality and chronic fatigue
- Difficulties with swallowing and verbal communication
Psychological and Social Impact
- Depression affects 40% patientsand is more common than in the general population
- Anxiety and fears related to the progression of the disease
- Loss of self-esteem and feelings of inadequacy
- Social isolation due to mobility difficulties (and the previous point)
- Social stigma associated with visible symptoms
Professional and Economic Impact
- 60% patients retire early
- Significant reduction in labour productivity
- Direct costs (medication, consultations) and indirect costs (care, loss of productivity)
- Growing need for home support and housing adaptations
- Financial and emotional burden on family carers

How is Parkinson's Disease treated?
The treatment of Parkinson's disease requires a personalised multidisciplinary approachcombining different therapeutic modalities to optimising symptomatic control and quality of life.
Multidisciplinary Approach
Ideal management involves a team which can include neurologist, neuropsychologist, physiotherapist, occupational therapist and speech therapist. This integrated approach makes it possible to address both motor symptoms (rigidity, tremor, bradykinesia...) such as the non-motorised (cognitive changes, sleep disorders, depression, anxiety...).
Pharmacological treatment
Drug treatment remains a fundamental pillarbased on the replacement or potentiation of dopaminergic activity.
Levodopa/Carbidopa
- It is the most effective drug, considered the "gold standard"
- Clearly improves stiffness and slowness of movement
- Over time, it can lose its effectiveness and cause involuntary movements (dyskinesias) or motor fluctuations, requiring dose adjustments.
Dopamine agonists
Drugs that directly stimulate dopamine receptors.
Main drugs:
- Pramipexole, Ropinirole (oral)
- Rotigotine (transdermal patch)
- Apomorphine (subcutaneous injection)
How they work:
- They directly stimulate dopamine receptors
- They are less potent than levodopa, but last longer and cause less dyskinesia at first
- They can cause unwanted effects such as drowsiness, swelling in the legs or changes in impulse control
Other Medicines
- MAO-B inhibitors (rasagiline, selegiline): neuroprotectants - help prolong dopamine in the brain
- COMT inhibitors (entacapone): prolong the effect of levodopa
- Amantadine: useful for controlling dyskinesias
- Anticholinergicsonly used in cases of persistent tremor in young patients
Neurotherapy in Parkinson's (non-invasive)
Neurotherapy is one of the approaches most promising and innovative in the treatment of Parkinson's, offering increases in well-being and neurological indices with a very high safety profile.
Transcranial Magnetic Stimulation (TMS)
EMT uses magnetic fields to modular the activity of specific brain areas related to the motor control e other functions affected in Parkinson's.
How it works:
- Non-invasive stimulation of the motor cortex and prefrontal areas
- Modulation of neuronal activity by magnetic fields
- High frequency protocols (10Hz) for stimulation or low frequency (1Hz) for inhibition
- 20-30 minute sessions, usually 5 times a week
Registered benefits:
- Significant improvement in bradykinesia and slowness of movement
- Reduced muscle stiffness
- Improved gait and reduced freezing
- Benefits for associated depressive symptoms
- Improved cognitive functions, especially executive functions
Advantages of EMT:
- Painless treatment
- No significant side effects
- Can be combined with medication and other therapies
- Effects continue for at least months after treatment - in addition to the definite impact on the treatment status of the condition
- Alternative for patients who can't tolerate medication
Deep Brain Stimulation (DBS)
Deep brain stimulation is a surgical option for Parkinson's patients advanced and motor complications significant.
In January 2020, the St John's Hospital became the 3rd hospital centre in the world to perform this surgerywith the implantation of a neuro-stimulator.DBS principles
A device implemented under the skin, in the chest, which works like a "brain pacemaker", he sends adjustable electrical impulses to specific brain nuclei.
Small electrodesimplanted in the brain, remain connected to the device senderserving as receivers.In New generation DBSthe electrodes receive and also "measure" signals from the brain, allowing you to adjust the stimulation in real time.Benefits and trade-offs:
- Can significantly reduce motor symptoms and allow medication to be reduced
- The benefits can last more than 10 years
- Like any surgery, there are risks (haemorrhage, infection, need to replace the battery)
In PortugalIt is estimated that around 1200 patients have already benefited from this intervention.
Physiotherapy and Rehabilitation
Exercise and physiotherapy are fundamental in all stages of the disease.
- They improve mobility, balance and gait.
- They help prevent falls and maintain independence.
- Therapies such as speech therapy and occupational therapy are equally important for quality of life.
In NeuroPsyque our commitment is, as always, to provide you with the greatest possible expectation of improvement.
We have the most specialised equipment and experts in areas such as Neurology and Neuropsychologyand also in therapies such as Transcranial Magnetic Stimulationwhich has proved important in the treatment of Parkinson's. Book your appointment with us!

When to seek professional help
O early recognition Parkinson's symptoms is crucial to initiate appropriate treatment and optimise long-term prognosis.
Warning signs
Seek specialised neurological assessment if observed:
- Resting tremor in a hand, arm or leg
- Progressive slowness of movement (bradykinesia)
- Muscle stiffness, especially in the morning
- Changes in gait (shorter steps, dragging feet)
- Decreased arm swing when walking
- Letter getting progressively smaller (micrograph)
- Lower or monotone voice
- Reduced facial expression ("face mask")
- Loss of sense of smell not related to constipation
Early Non-Motor Symptoms
- REM sleep disorders (moving during dreams)
- Persistent constipation
- Depression or anxiety with no apparent cause
- Excessive fatigue
- Mild cognitive impairment
When it's Urgent
Search immediate medical help se:
- Several Parkinson's symptoms appear suddenly (may indicate secondary parkinsonism)
- Frequent falls or marked postural instability
- Develops hallucinations or confusion
- Severe dysphagia (difficulty swallowing)
- Severe "freezing" (paralysis) occurs with prolonged episodes of immobility
Importance of Early Diagnosis
- Allows neuroprotective treatment to begin
- Better initial response to medication
- Possibility of delaying complications
- Proper family and career planning
- Access to social support and rehabilitation programmes
How to deal with Parkinson's in everyday life?
Living with Parkinson's requires specific adaptations and strategiesBut many people maintain an active and satisfying life for many years after their diagnosis.
Movement and Activity Strategies
- Regular exercise: Physical activity is essential - walking, swimming, tai chi, dancing...
- Specific exercises and techniques: Wide movements, voice exercises (methods LSVT BIG e LSTV LOUD)
- Physiotherapy specialised: Specific techniques for Parkinson's
- Break freezing: Visual, auditory and tactile techniques
- Security at home: Removal of carpets, installation of support bars...
Medication Management
- Taking medication at the exact times prescribed
- Keep a diary of symptoms and response to medication
- Never stop medication abruptly
- Report side effects to the doctor
Sleep Care
- Keeping regular bedtimes and getting up times
- Create an environment conducive to rest (dark, quiet, suitable temperature)
- Avoid caffeine after 2pm
- Relaxation techniques before bed
- Treat REM sleep disorders if present
Nutrition and Food
- Balanced diet rich in fibre (for constipation)
- Adequate hydration
- Avoid high-protein meals when taking levodopa
- Vitamin supplementation - when indicated
- Dietary adaptations to overcome swallowing difficulties
Psychological and social support
- Staying socially active
- Participate in support groups
- Communicate openly about the condition
- Seek psychological support when necessary
- Keep hobbies and pleasurable activities adapted
Practical adaptations
- Wear clothes with Velcro instead of buttons
- Shoes without laces or with elasticated laces
- Adapted kitchen utensils
- Phone with large buttons
- Mobile applications (reminders) to remember medication

Advances in scientific research
Parkinson's research is ongoing constant evolutionThis has brought renewed hope for better treatment, prevention and eventually a cure for the disease.
Emerging Therapies
- Immunotherapyuse of antibodies (such as prasinezumab e cinpanemab) that target protein α-synuclein, accumulated in the brain cells of people with Parkinson's.
- Gene therapyThis is done by introducing genes that stimulate the production of enzymes related to dopamine, a substance that is essential for controlling movement.
- Stem cellstransplantation of cells capable of transforming into dopamine-producing neurons.
- GLP-1 inhibitorsdrugs already used in diabetes that show potential for protecting brain cells.
- Intestinal microbiome: study of specific probiotics to balance the relationship between the gut and the brain.
Genetic Research
- More from 20 genes associated with Parkinson's have already been identified.
- Therapies are being developed to target specific mutations, such as in genes LRRK2 e GBA.
- A personalised medicine is starting to use each patient's genetic profile to guide treatment.
- In Portugal, studies are being carried out on families carrying the mutation LRRK2.
New Biomarkers
Biomarkers are biological signals that help in the early diagnosis and monitoring of the disease.
- α-synuclein in cerebrospinal fluid (cerebrospinal fluid) can enable a diagnosis to be made before motor symptoms appear.
- Blood tests study inflammatory proteins and neurofilaments as possible markers.
- Advanced neuroimaging (PET and functional MRI) helps identify early brain changes.
- Digital biomarkersTests are already underway, such as analysing gait or voice via mobile applications.
Personalised Medicine
- Stratification of patients according to molecular subtype of the disease.
- Treatments that are increasingly adapted to specific cause of Parkinson's in each person.
- Possibility of predicting individual therapeutic response.
- Strategies for prevention in people with a high genetic risk.
Technology and Devices
- Intelligent deep brain stimulation (DBS)with systems that adapt stimulation in real time.
- Metering devices who continuously monitor symptoms.
- Use of virtual reality in motor and cognitive rehabilitation programmes.
- Application of artificial intelligence to optimise therapies and predict disease progression based on the patient's profile.
Myths and Truths about Parkinson's
It's essential debunking misconceptions about Parkinson's that can generate stigma and delay proper treatment.
| Myth | Truth |
| "Parkinson's is uncontrolled tremor" | Parkinson's has multiple motor and non-motor symptoms. 20-30% of patients never develop significant tremor. |
| "It only affects elderly people" | Although more common after the age of 60, 5-10% of cases start before the age of 50. The youngest diagnosed was 18 years old. |
| "It's a death sentence" | Parkinson's is not fatal in itself. With proper treatment, life expectancy can be almost normal. |
| "The medication is toxic and should be avoided" | Modern medication is safe and effective. The benefits far outweigh the risks in most cases. |
| "Exercise is dangerous" | Controlled exercise is extremely beneficial. It improves motor symptoms, mood and quality of life. |
| "It's always hereditary" | Only 10-15% have a clear familial component. Most cases are sporadic. |
| "Nothing can be done" | There are many effective therapeutic options, including medication, neurotherapy, DBS and rehabilitation. |
| "It affects intelligence" | Intelligence remains preserved in most cases. Cognitive decline, when it occurs, is late. |
Resources and support available in Portugal
Portugal has a growing network of specialised resources for people with Parkinson's and their families.
| Resource | Description | Contact |
| Portuguese Association of Parkinson's Disease (APDPk) | National organisation dedicated to supporting, informing and defending rights | www.parkinson.pt |
| National Health Service (SNS) | Neurology and physical medicine consultations through the family doctor | Local health centre |
| SNS 24 line | 24-hour telephone support for health issues | 808 24 24 24 |
| Local Support Groups | Regular meetings to share experiences | Through APDPk |
| Special Medicines Programme | Reimbursement for Parkinson's medicines | Hospital pharmacies |
| Social Support | Dependency supplement, tax exemptions | Social Security |
Rights and Specific Support
- Recognising disability (≥60%) confers tax and social benefits
- Exemption from user charges for consultations and medicines
- Possibility of early retirement due to disability
- Adaptations to the workplace according to Law no. 38/2004
- Priority in booking specialised appointments
Conclusion
Parkinson's disease is a neurological condition complex which profoundly affects the lives of around 20,000 Portuguese and their families. Although it is progressive and currently incurableIt is essential to emphasise that there are multiple effective therapeutic options that can provide a good quality of life for many years.
Essential key points:
Early diagnosis is crucial to optimise treatment and slow progression. The initial symptoms can be subtlebut timely identification allows therapeutic measures to be initiated that make a significant difference in the evolution of the disease.
Treatment options have expanded dramatically in recent decades. In addition to classic dopaminergic medication, we now have advanced neurotherapy, deep brain stimulation, and multidisciplinary approaches that address both motor and non-motor symptoms.
O regular physical exercise and specialised physiotherapy are as important as medication in managing the condition. Scientific evidence clearly demonstrates that adapted physical activity improves symptoms, slows progression and increases quality of life.
Family, social and psychological support is fundamental. Living with Parkinson's is a challenge that is much better faced with the support of family and friends, with understanding, adaptation and optimism based on the real therapeutic possibilities available.
Scientific research continues to bring hope. We are in a era of accelerated discoverywith gene therapies, immunotherapies and personalised medicine on the near horizon. Portugal is actively contributing to this research, especially in genetic studies.
A message of hope:
The diagnosis of Parkinson's it's not a definitive judgement. With proper treatment, specialised monitoring and the right strategies, it is possible to maintain an active, productive and satisfying life. Each person is unique, and finding the ideal therapeutic combination may take time and adjustments, but it's worth persevering.
In NeuroPsyquewe work every day to give the best possible expectation of improvement for our patientsusing a truly integrated approach that combines the best of Neurology, Neuropsychology, e Advanced neurotherapy.
FAQ's about Parkinson's
1. Is Parkinson's curable?
There is currently no cure (the complete and definitive elimination of the disease, with no possibility of it returning) for Parkinson's, but the symptoms can be very well controlled with appropriate treatment. Research into curative treatments is very active.
2. What is the difference between tremor and Parkinson's?
Not all tremor means Parkinson's. In Parkinson's, tremor appears at rest and decreases with movement. Essential tremor occurs during action. The diagnosis of Parkinson's requires bradykinesia (slowness) and tremor or rigidity, not just tremor alone.
3. How is Parkinson's diagnosed?
Diagnosis is mainly clinical, based on history and neurological examination. There is no definitive test. The neurologist assesses motor symptoms, response to levodopa, and rules out other causes.
4. Is neurotherapy effective for Parkinson's?
Yes. Transcranial Magnetic Stimulation shows significant benefits in bradykinesia, rigidity, gait and non-motor symptoms. It is a safe alternative with fewer side effects than medication, and can be combined with other treatments.
5. When is DBS surgery indicated?
Deep brain stimulation is considered when there are motor fluctuations or dyskinesias that do not respond to medication, usually after 5-10 years of illness. The patient must have a good historical response to levodopa and absence of severe dementia.
6. Does Parkinson's affect intelligence?
Not directly. Most people maintain normal intelligence. There may be slight alterations in attention and executive functions, especially in advanced stages, but basic intelligence is preserved in the vast majority of cases.
7. Is Parkinson's disease hereditary?
Only 10-15% of cases have a clear familial component. Most cases result from the interaction between genetic predisposition and environmental factors. Having a relative with Parkinson's slightly increases the risk, but does not determine that you will develop the disease.
8. How to deal with "off periods"?
"Off" periods (when medication loses effect) can be managed with: medication timing adjustments, long-acting dopamine agonists, COMT inhibitors, movement techniques to break freezing, and in severe cases, DBS or apomorphine pumps.
9. Does exercise help with Parkinson's?
Absolutely essential. Exercise is one of the best "medicines" for Parkinson's. It improves strength, balance, gait and mood and can slow down progression. Wide-ranging exercises, dancing, non-contact boxing and aquatic activities are especially beneficial.
10. What are the side effects of the medicines?
Levodopa can cause dyskinesias (involuntary muscle movements) and motor fluctuations after years of use. Dopamine agonists can cause drowsiness, oedema, hallucinations and impulse control disorders. Most effects are dose-dependent and reversible with adjustments.
11. Is young onset Parkinson's different?
Yes. Parkinson's before the age of 50 generally has a slower progression initially, a greater genetic component, and has a higher risk of early dyskinesias (involuntary muscle movements) with levodopa. They often benefit from dopamine agonists as the first line of treatment.
12. Are there any support groups in Portugal?
Yes, the Portuguese Parkinson's Association (APDPk) coordinates regional groups. There are also informal groups in various cities and online platforms. Local support is essential for sharing experiences and practical strategies.




2 responses
My husband was diagnosed of Parkinsons disease 2 years ago, when he was 49. He had a stooped posture, tremors, right arm does not move and also a pulsating feeling in his body. He was placed on Senemet for 8 months and then Sifrol was introduced and replaced the Senemet, during this time span he was also diagnosed with dementia. He started having hallucinations, lost touch with reality. Suspecting it was the medication I took him off the Siferol (with the doctor's knowledge) and started him on PD-5 natural herbal formula we ordered from AKNNI HERBAL CENTRE, his symptoms totally declined over a 3 weeks use of the AKANNI HERBAL Parkinson's disease natural herbal formula. He is now almost 51 and doing very well, the disease is totally reversed! (Visit w w w.aknniherbscentre .com)
I was diagnosed with Parkinson's disease a year ago at the age of 67. For several months I had noticed tremors in my right hand and the shaking of my right foot when I was sitting. My normally beautiful cursive writing was now small, cramped printing. And I tended to lose my balance. The neurologist had me walk down the hall and said I didn't swing my right arm. I had never noticed! I was in denial for a while, as there is no history in my family of parents and five older siblings, but I had to accept I had classic symptoms. I was taking amantadine and carbidopa/levodopa and was about to start physical therapy to strengthen muscles. I used different supplements that didn't work, so last July, I tried the PD-5 protocol-the best decision ever! My tremors eased, my energy returned, and I sleep soundly. I feel like a new woman, and I can walk and exercise again. I got the PD-5 from ww w. limitless healthcenter. co m