Around 3 in 10 Portuguese have been diagnosed with depression, and more than half, 6 in 10, have experienced depressive symptoms at some point in their lives. The real figures, with cases that never reach the doctor's office, are estimated to be even higher. But what is depression really? Is it just a prolonged feeling of sadness?
Around 3 in 10 Portuguese have been diagnosed with depression, and more than half, 6 in 10, have experienced depressive symptoms at some point in their lives. The real figures, with cases that never reach the doctor's office, are estimated to be even higher. But what is depression really? Is it just a prolonged feeling of sadness?
It's waking up and needing 15 minutes just to find the energy to get up. It's smiling automatically when someone asks how you are, because explaining that "everything is in order but nothing makes sense" is too complicated.
It's the guilt of feeling this way when "life isn't so bad". It's cancelling plans for the third time because you can't find the words to explain that getting out of bed today was a victory. It's hearing "you need to cheer up" and knowing that the person saying it doesn't understand that it's not a question of willpower - it's like asking someone with a broken leg to run a marathon.
For those living with depression, it's not a lack of toughness, or just something "psychological".
It's a disease that has a tremendous impact on the way you live and interact with others, that alters your perception of the passage of time, and even makes your strongest likes and desires irrelevant.
Let's dive into what we know about Depression, and try to understand it in order to better treat it.
What is Depression?
Depression is a mental disorder that affects the humour, the thoughts, o behaviour and physical well-being. It differs greatly from passing sadness, laziness or lack of willpower.
Today is main cause of disability in the world.
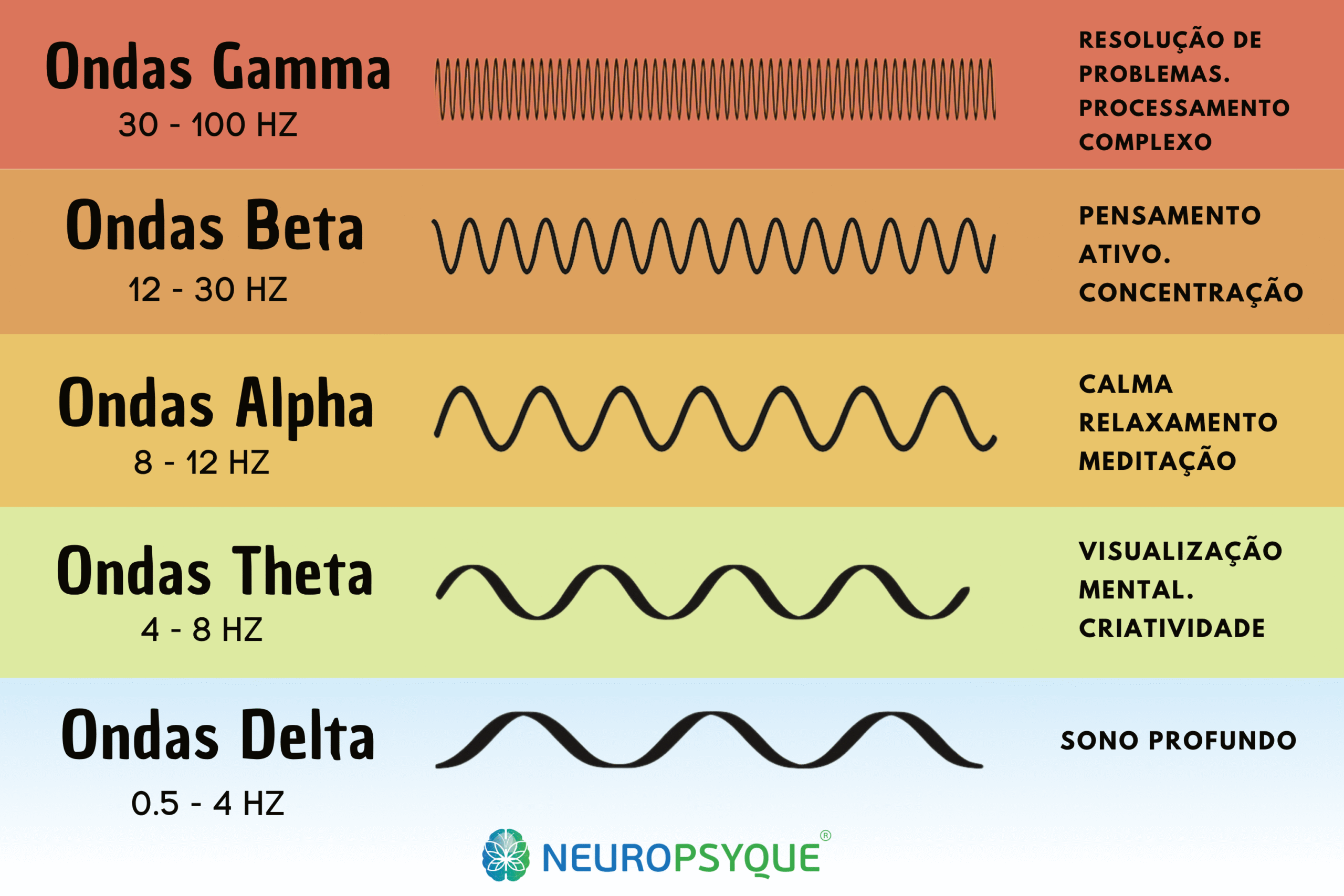
The brain of a person with depression shows some measurable changes.
Levels of neurotransmitters such as serotonin, noradrenaline e dopamine are dysregulated. Areas responsible for emotional regulationsuch as prefrontal cortex and limbic system, show altered activity.
Depression is too, but not only:
- Being sad after a negative event
- Tiredness or laziness
- Lack of will
Depression is and contains:
- Persistence of symptoms (+ 2 weeks)
- Impact on daily functionality in various environments
- Neurological and chemical changes in the brain
- Signs that are difficult to distinguish from mere sadness
The figures are clear: at least one in four or five people will experience depression in their lifetime. This means that you probably know someone who is going through it or has gone through it. Or maybe you're going through it right now.
It's very important that we understand this condition as much as possible - Throughout our lives, we can help ourselves, those close to us and thousands of people we come across.
Depression affects all areas of life. Work, relationships, physical health, the ability to feel pleasure. For some people, even the simplest day-to-day tasks become mountains.
A World Health Organisation (WHO) classifies International Classification of Diseases (ICD-11), various types of depressive disorders.
Types of Depression
Depression is not the same for everyone. There are different types, each with its own characteristics.
Understanding the type of depression is fundamental to finding the most appropriate treatment.
Major Depressive Disorder
This is the most common type. It is characterised by intense depressive episodes that can be one-off or recurrent. The symptoms are severe and seriously interfere with daily life.
Some people only have one episode in their lives. Others experience several over the years.
Persistent Depressive Disorder (Dysthymia)
The symptoms are less intense than in major depression, but they are chronic. They last at least two years, often decades.
It's like living permanently with a weight on your shoulders. There are better days and worse days, but you're never truly well.
There are cases in which, in addition to this type, there are overlapping episodes of major depression, in a condition called "double depression".
Depression with Melancholic Characteristics
It is marked by a total inability to feel pleasure or any kind of satisfaction, even temporarily. Nothing can improve the mood, even for a moment.
Symptoms are typically worse in the morning. Waking up is particularly difficult.
There are visible psychomotor changes: very slow movements or, on the contrary, marked agitation. Significant loss of appetite and weight. Deep feelings of guilt.
Atypical Depression
The name is misleading: it's quite common. The main characteristic is "mood reactivity" - the ability to temporarily feel better when something positive happens.
Other symptoms include increased appetite and weight, excessive need for sleep (hypersomnia), a feeling of heaviness in the arms and legs, and extreme sensitivity to rejection.
This sensitivity can profoundly affect relationships.
Premenstrual Dysphoric Disorder
It goes far beyond the common premenstrual syndrome. The depressive symptoms are severe and appear the week before menstruation.
They improve significantly after the start of the cycle. They include intense depressed mood, anxiety, irritability, and marked interference with work and relationships.
Psychotic Depression
It occurs when severe depression is accompanied by delusions or hallucinations. The content is usually negative: ideas of guilt, ruin, serious illness or punishment.
It always requires urgent specialised treatment.
Postpartum Depression
It appears after birth and is very different from the normal "baby blues". It affects the ability to look after the baby and to function.

Symptoms and Manifestations of Depression
Depression doesn't just affect mood - it affects body and mind, and alters habits, routines and behaviours over time.
Emotional Symptoms
Persistent Depressed Mood
It's not just sadness - many people describe it as emptiness, an absence of feeling. Grey days even when the sun is shining.
Generalised Loss of Interest (Anhedonia)
Anhedonia is central: loss of interest or pleasure in activities that used to give satisfaction. Hobbies abandoned, invitations refused, indifference to things that used to matter.
Constant feeling of guilt
Feelings of guilt, worthlessness or inadequacy are common. The person feels like a burden to others. Everything seems to be their fault, even when it clearly isn't.
Loss of Hope
Hopelessness sets in. The future looks bleak, with no possibility of improvement.
Irritability
Small setbacks provoke disproportionate reactions.
Cognitive symptoms
Concentration difficulties
Concentration is compromised. Reading an article, following a film, holding a conversation - everything requires more effort.
Memory failures
Memory fails. Frequent forgetfulness creates a feeling of frustration.
Inability to Make Decisions
Simple decisions become impossible. "What will I have for lunch?" can generate paralysing anxiety.
Reduced Reaction Time and Slow Thinking
Thinking becomes slow. Words don't come easily. Processing information takes longer.
Thoughts Related to Death
Recurrent thoughts of death or suicide can arise. From passive wishes ("I wish I didn't wake up") to suicidal ideation with planning.
Physical symptoms
Insomnia or hypersomnia
Sleep disorders are very common. Insomnia (difficulty falling asleep, frequent awakenings, early waking) or the opposite - hypersomnia, sleeping 12, 14, 16 hours and still being exhausted.
Significant loss or gain of appetite
Appetite changes. Some people lose interest in eating completely, losing significant weight. Others develop binge eating, gaining weight.
Constant Fatigue
The fatigue is constant. It's not the normal kind of tiredness that improves with rest. It's deep exhaustion, present from the moment you wake up.
Pain and discomfort with no obvious cause
Physical pains with no apparent medical cause are common. Headaches, muscle aches, gastrointestinal discomfort.
Psychomotor slowness and/or hyperactivity
Movements and speech can become visibly slow (psychomotor slowing) or constant agitation can appear - an inability to sit still.
Loss or Disappearance of Libido
Libido decreases or disappears.
Summary table
| Category | Main symptoms |
| Emotional | Depressed mood, anhedonia, guilt, hopelessness, irritability |
| Cognitive | Difficulty concentrating, memory problems, indecisiveness, slow thinking, suicidal ideation |
| Physical | Sleep changes, appetite changes, fatigue, pain, slowing down/agitation, decreased libido |
Temporal Patterns
Depression can be persistent, cyclical or seasonal.
A persistent depression no intervals of well-being or significant symptom relief.
A cyclical depression shows large, repeated oscillations, with big differences between the highs and lows.
A seasonal depression is associated with the season, often worsening in autumn/winter and improving in spring/summer.
As for the demonstrations throughout the dayThere are also big differences.
In melancholic depressionThe symptoms are typically worse in the morning. Waking up is the hardest part of the day.
There can be a lot of variation throughout the day. Some people feel a slight improvement in the evening, for example, while others experience distress associated with insomnia, and the anxiety of having to get up early the next day.
Urgent warning signs
Some symptoms are especially seriousand therefore demand immediate action:
- Suicidal thoughts with ideation and concrete planning
- Intention to harm yourself (self-mutilation)
- Serious neglect of self-care (not eating, not drinking water, total neglect of daily hygiene)
- Prolonged isolation at home (+ 14 days without physical contact with the outside)
- Psychotic symptoms (delusions, hallucinations)
- Total inability to function or prolonged hypersomnia (+14 days with daily sleep of more than 10 hours)

Causes and Risk Factors
Depression no single cause. It results, as with almost all neuropsychiatric conditions, from the complex interaction between biological factors, psychological e social.
As well as some of these factors being consequences of depression, arising from other causes, they can be directly or indirectly, and usually together, causative of the condition.
Biological factors
Genetics
Having a close relative with depression increases the risk 2-3 times. But genetics is not destiny - many people with a family history never develop the condition.
Neurochemical changes
Imbalances in neurotransmitters (serotonin, noradrenaline, dopamine) are well documented and associated with the condition. These chemicals regulate mood, motivation and pleasure.
Changes in Brain Structure
Neuroimaging studies show differences in the hippocampus, amygdala and prefrontal cortex of people with depression.
Hormonal dysfunctions
The brain structure that regulates the stress response (hypothalamic-pituitary-adrenal axis) functions abnormally in many cases of depression.
Psychological factors
Negative Beliefs and Thought Patterns
Negative thought patterns increase vulnerability to the expansion of the condition. Seeing yourself, the world and the future through a negative lens creates a self-perpetuating cycle.
Insecurities
Low self-esteem, rigid perfectionism and a tendency to blame yourself for everything create fertile ground for depression.
Traumas
Psychological trauma, especially in childhood, leaves deep scars. Abuse, neglect or significant losses increase the risk.
Social and Environmental Factors
Stressful life events and pathological (chronic) stress are often the trigger:
- Grief and loss
- Separation or divorce
- Job loss or financial difficulties
- Health problems, their own or of people close to them
- Drastic life changes
- Serious relational conflicts
Social isolation is both a cause and a consequence. The lack of social support increases vulnerability and the likelihood of prolonged suffering. It is very important to maintain a network of close people, and to talk about your state of mind and the difficulties you are facing.
Demographic factors in Portugal
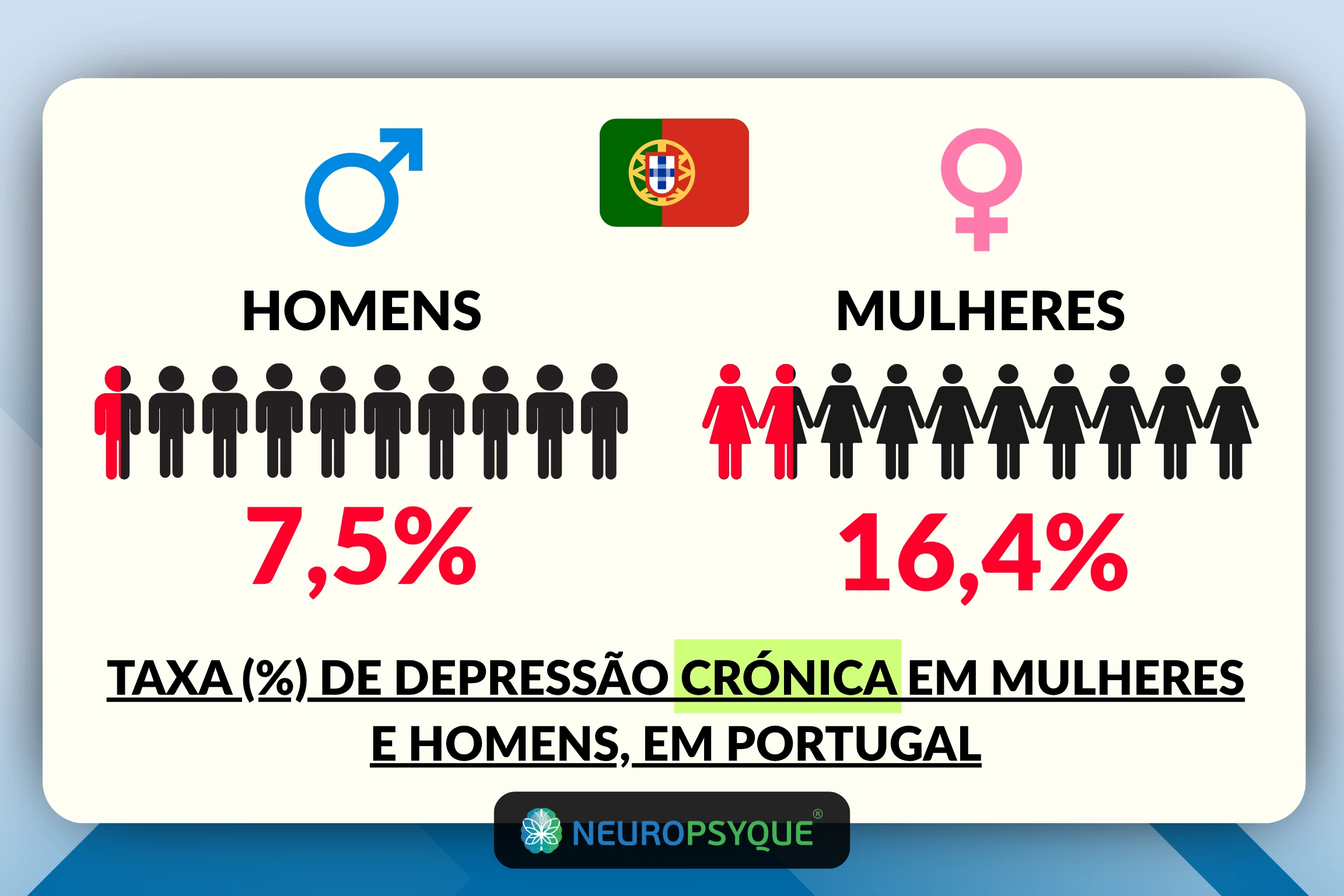
Women are significantly more affected: 16,4% suffer from chronic depressionin the face of 7,5% of men. This is the biggest disparity in Europe in the figures for depression.
Socio-economic status has a big impact. People with low incomesThis represents a large slice of the Portuguese population, with higher rates of depression and often difficulties in getting the help and support they need.
Associated Medical Conditions
Various physical illnesses increase the risk of depression. Some are often associated:
- Oncological diseases (cancer)
- Cardiovascular diseases
- STROKE
- Parkinson's disease
- Chronic pain
- Diabetes
- Thyroid disorders
There are some drugs used to treat other health conditions that are associated with and can trigger or aggravate depression: drugs for hypertension, statins, corticosteroids, etc.
The Diagnosis of Depression
The diagnosis of depression is clinical. There is no blood test or brain scan to confirm the condition.
The diagnosis is made by a psychiatrist or clinical psychologist through a careful assessment.
The Diagnostic Process
The consultation begins with a detailed interview (anamnesis). The professional asks you about your symptoms: what you feel, since when, and how it affects your life.
A research personal and family history, recent life events, medication you take or have taken, etc.
O mental state examinationThis frequently used tool assesses mood and patterns of thought and behaviour. How you speak, how you move, how you interact.
Laboratory tests can be ordered - not to diagnose depression, but to exclude other medical causes, and eventually help distinguish between types. Thyroid problems, for example, can cause similar symptoms.
DSM-5 criteria
O Diagnostic and Statistical Manual of Mental Disorders (DSM-5) establishes specific criteria for diagnosing the most common type, the Major Depressive Disorder:
You need 5 or more of the following symptoms over the same two-week period:
- Negative mood most of the day, almost every day
- Marked loss of interest or pleasure
- Significant change in weight or appetite
- Insomnia or hypersomnia almost every day
- Observable psychomotor agitation or slowing down
- Fatigue or loss of energy
- Feelings of worthlessness or excessive guilt
- Decreased ability to think or concentrate
- Recurrent thoughts of death or suicide
At least 1 of the following symptoms must be present:
- Negative mood
- Loss of interest or pleasure
The following 3 points must also be checked:
- Symptoms cause significant suffering or functional impairment
- Not attributable to chemical substances or another medical condition
- Never had a manic or hypomanic episode
Gravity
Apart from the types that are always severe, such as psychotic depression, there are different levels of intensity assigned to the diagnosis. Here are the 3 classifications:
Lightweight: Few symptoms beyond the minimum necessary for diagnosis. Functional impairment (in day-to-day life) is slight.
Moderate: Mild to severe symptoms and impairment.
Serious: Almost all symptoms present. Very marked impairment of activities. May include psychotic features.
Assessment instruments
Different standardised scales are used internationally to help quantify severity in order to guide treatment. Here are a few:
These tools don't diagnose on their own, but they do help the professional.
Challenges
In Portugal, the interval between onset of symptoms and medical treatment is, on average, five years. It's too long.
Only 25 to 35% of people with depression seek medical attention within the first year of symptoms.
The stigma is still enormous. Many people find it difficult to recognise that they are ill or feel ashamed to seek help. The work of awarenesswhich removes the barrier of shame, and saving lives every day.
Depression in Children and Adolescents
In younger people, depression can manifest itself differently. Irritability usually predominates over sadness as the most visible symptom. Behavioural problems or school performance can be signs of the condition.
Specialised assessment is crucialThe criteria should always be adapted to age.

Impact of Depression on Daily Life
At work or study:
- Frequent absences (absenteeism)
- Being present but not producing (presentism)
- Difficulty concentrating
- Most common mistakes
- Relationships with colleagues deteriorate
- Real risk of losing your job or dropping out of school
In social relations:
- Progressive insulation
- Constant cancellation of appointments
- Friendships are lost through lack of contact
- Feeling of incomprehension: "nobody understands"
- Difficulty explaining their feelings
- Guilt for "disappointing" others
In the family:
- Tension in relationships with spouse or partner
- Difficulty in fulfilling domestic responsibilities
- Impact on children (if any)
- Intense feelings of guilt for "not being enough"
- Conflicts increase
Physical health:
- Increased risk of cardiovascular disease and stroke
- Compromised immune system
- Aggravation of existing medical conditions (diabetes, hypertension...)
- Neglect of basic self-care
In mental health:
- Frequent comorbidities: anxiety in around half of cases
- Risk of substance abuse (compulsions or self-medication)
- Suicide risk: in 70% of suicides, depression is involved
Untreated depression tends to get worse over time. The consequences accumulate and the suffering intensifies.
But there is hope. Thoughtful and careful treatment works. It's imperative that you never stop believing in better times.
How is Depression treated?
Unlike other neurologically-based conditions, depression is a treatable condition - it can be treated. complete remission of symptoms is possible. In many cases, the symptoms never return.
The most effective approach combines always different therapies, adapted to the specific case and its specific needs.
Pharmacological treatment
Antidepressants are medicines used for mild to severe depression. Here are some of the most commonly used:
SSRIs (Selective Serotonin Reuptake Inhibitors)
They are usually the first choice. They include fluoxetine, sertraline, escitalopram, paroxetine.
They increase the availability of serotonin, a neurotransmitter responsible for regulating a wide range of functions in the body, especially in the brain. Regulation of mood, sleep-wake cycles, appetite and digestion, concentration and memory, pain and even the immune system.
SNRIs (Serotonin and Noradrenaline Reuptake Inhibitors)
Venlafaxine and duloxetine. In addition to serotonin, they act on the availability of noradrenaline. Noradrenaline is an "accelerator" of the body and mind - it is essential for maintaining alertness, energy and motivation, and the ability to concentrate.
Tricyclic Antidepressants
Amitriptyline, imipramine, clomipramine, nortriptyline. They are used when SSRIs and NRTIs do not have the desired efficacy. Although effective, they tend to have more side effects.
MAOIs (Monoamine oxidase inhibitors)
For use in specific cases - they require special dietary care. They prevent the action of this enzyme, monoamine oxidase, which breaks down neurotransmitters such as serotonin, noradrenaline and dopamine, the abundance of which improves mood.
Common Side Effects and Important Notes
The therapeutic effect of antidepressants it's not immediate. They are necessary 2 to 4 weeks to feel the first positive effects.
It is essential to take it as prescribed, even when you start to feel better. Stopping abruptly can cause discontinuation symptoms.
Here are some of the most common side effects:
- Nausea
- Gastrointestinal problems
- Sexual dysfunction
- Anxiety
- Insomnia/somnolence
- Weight gain
- Headaches
Always report these and other unwanted effects to your doctor so that you can readjust your treatment. Close contact with your doctor is of the utmost importance.
Psychotherapy
A Psychotherapy and psychological counselling are fundamental in the treatment of depression. For mild to moderate cases, it can be enough on its own.
Cognitive Behavioural Therapy (CBT)
It is the psychological therapy with the most scientific evidence for depression. It is classified as a first-line treatment.
CBT helps identify and modify negative thought patterns. These automatic thoughts, which emerge from the subconscious ("I'm a failure", "nothing will ever get better", "nobody likes me"), feed and maintain depression.
Here are some practical strategies that are widely used:
- Recognising distorted thoughts
- Question the validity of these thoughts
- Develop more realistic alternative perspectives
- Solve problems in a structured way
- Activate positive behaviours and reactions
Behavioural activation is especially important.
Depression generates a vicious circleFeeling bad leads to doing less and fear of failure, and doing less reduces sources of pleasure and satisfaction, which aggravates depression.
Breaking this cycle by gradually resuming activities is fundamental.
The typical CBT lasts 12 to 20 sessionsBut many people keep psychotherapy as a habit forever, because of the benefits they recognise in it.
Interpersonal Therapy (IPT)
This type of therapy focuses in detail on relationships and life transitions. It is particularly effective when depression is related to:
- Grief or loss
- Interpersonal conflicts
- Role transitions (retiring, becoming a parent...)
- Deficits in social skills
It's an average therapy 12 to 16 weekswith clear objectives and structured progression.
Other Psychological Approaches
Problem-solving therapy, Mindfulness, and Acceptance and Commitment Therapy also show excellent effectiveness.
Neurotherapy - Transcranial Magnetic Stimulation
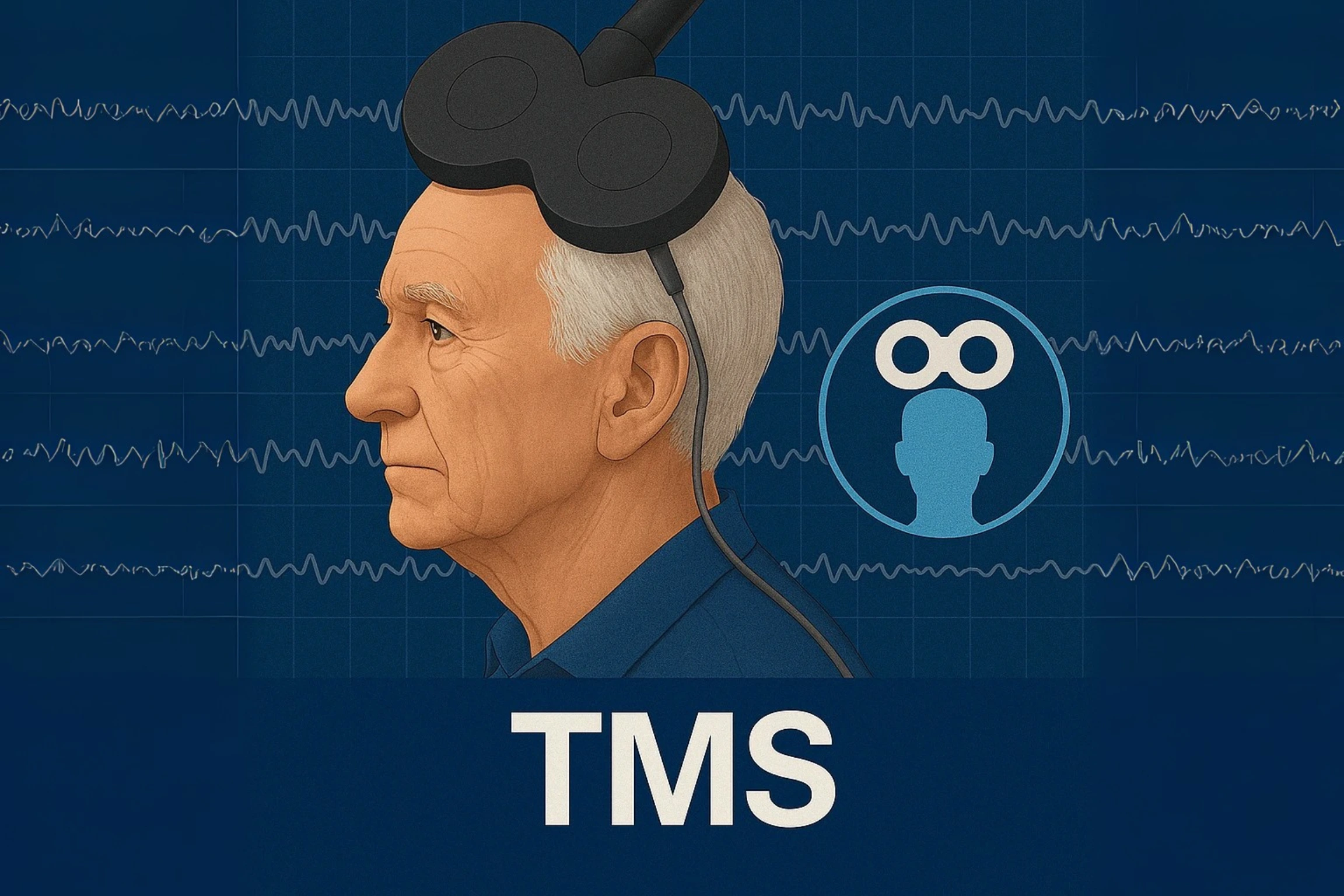
Transcranial Magnetic Stimulation (EMT) represents a significant advance in the treatment of depression. It is a non-invasive (non-surgical) and painless technique, with very high efficacy rates and close to 0 (zero) incidence of side effects. It has level A scientific evidence for the treatment of depression - the highest rating.
How it works
A EMT utilises magnetic pulses to stimulate specific areas of the brain. A coil is placed next to the head, generating a magnetic field that passes painlessly through the skull.
The target is usually left dorsolateral prefrontal cortex - a key area in mood regulation. In people with depression, this region shows reduced activity.
Magnetic pulses modulate neuronal activity and balance levels of neurotransmitters such as serotonin, noradrenaline and dopamine. What's more, promote brain plasticity - the brain's ability to reorganise itself and create new connections.
For whom it is suitable:
- Preference for non-pharmacological treatment: Those looking for alternatives without medication.
- Treatment-resistant depression: Around 30% of people do not respond adequately to antidepressants. For these cases, EMT has proved to be very effective.
- Drug intolerance: People who cannot tolerate the side effects of antidepressants.
- Complementary treatment: It can be combined with psychotherapy and pharmacotherapy for superior and especially longer-lasting results.
Treatment
Each session lasts between 20 to 40 minutes. No anaesthesia or sedation required.
The person is awake and alert throughout the procedure and can continue with their normal activities immediately afterwards.
Improvement usually comes between the first and second week.
Studies show increasing response rates with the optimised protocols developed in recent years.
Security
EMT is safe and well tolerated. Here you can see a comparison of efficacy and side effect rates with pharmacological therapy. Side effects are minimal - occasionally mild discomfort at the application site or a slight headache.
It doesn't have the typical side effects of antidepressants (weight gain, sexual dysfunction, drowsiness, etc.).
In NeuroPsyque our commitment is, as always, to provide you with the greatest possible expectation of improvement.
We have the most specialised equipment and experts in areas such as Neurology, a Psychiatry and Neuropsychologyand also in therapies such as Transcranial Magnetic Stimulationwhich has proved central in the treatment of depression. Book your appointment with us!

When to seek professional help
Knowing when to seek help can save lives.
You should seek help if:
- Symptoms of depression persist for more than two weeks
- The ability to work, study or maintain relationships is compromised
- Basic daily tasks have become very difficult
- He's progressively isolating himself
- There are recurring thoughts of death or suicide
- You're using alcohol or substances to deal with your feelings
- Persistent physical symptoms with no identified medical cause
- Family or friends express concern
Help is urgently needed now, immediatelyif:
- You have suicidal thoughts with concrete planning
- You intend to get hurt
- Psychotic symptoms (delusions, hallucinations)
- Is in serious neglect of self-care
- You feel you're in danger
Emergency contacts
- 112 - National Emergency Number (24h)
- 1441 - National Suicide Prevention and Psychological Support Line
- SNS 24: 808 24 24 24 (option 4 for psychological support) (24h)
- SOS Friendly Voice: 213 544 545 | 912 802 669 | 963 524 660 | 800 209 899 (15.30 - 00.30)
- Conversa Amiga: 808 237 327 | 10 027 159 (3pm - 10pm)
- Friendly Voices of Hope from Portugal: 222 030 707 (4pm - 10pm)
- Friendship telephone number: 222 080 707 (4pm - 11pm)
- Voice Support: 225 506 070 | sos@vozdeapoio.pt (21h - 00h)
Whatever level of suffering you're carrying, don't expect things to get better on their own. Untreated depression tends to get worse. The sooner treatment begins, the better the prognosis.
Seeking help is definitely not a sign of weakness - it's a sign of courage to break the inertia, which has a lot of strength and requires more strength to break.

How to Deal with Depression in Everyday Life
There are conditions whose treatment depends almost entirely on what is done and defined in the consulting room.
This is not the case in the treatment of depression.
A large part of the improvement will happen outside the office. That's why two things are so important:
- The work inside the consulting room orientated and thinking about the preparation of the work that is done outside it
- The dedication and drive with which we "attack" the pillars of life with the greatest potential for improvement (which we will now address)
Routine and Structure - One Victory at a Time
Try to keep regular bedtimes and wake-up times. Even if you don't sleep well, get up at the same time.
Set small daily goals. "Today I'm going to take a shower" or "Today I'm going to go out for 10 minutes" are valid and important goals.
Breaking down large tasks into smaller steps can be essential in the process. The small victories accumulate and are a driving force for motivation.
Celebrate the small achievements. You don't have to climb the mountain all at once. Did you get out of bed when it was extremely difficult? That's a real victory. One victory at a time.
Medicine is Movement | Movement is Medicine
Physical exercise, as well as being a primal need, has an invaluable power for health and well-being in the long term, and has a proven antidepressant effect in the short term.
There are no formulas or rigid protocols that you have to follow.
Intense or not so intense; static or moving; in a group or alone, listening to music or meditating... choose what you like to do, what challenges you and allows you to make exercise a necessity that you can't avoid.
30 minutes of daily walking makes a difference. Even if you do other types of physical activity, consider walking to relax and meditate.
Start slowly if you're not used to it. Five minutes counts. Then gradually increase.
Conscious and Consistent Eating
Try to eat regular meals, even if you're not hungry. The body needs fuel.
Try to learn about nutrition and the body's functional needs.
A diet rich in protein and healthy fats is, in most cases, the best option. Avoid excess sugar at all costs, and moderate caffeine consumption.
Get to know them biomarkersIt is also important to make sure that your body is properly hydrated, through analyses (blood tests, for example), so that you can work with a professional to make up for any gaps in nutrients. Adequate hydration is also essential.
Rest as a Priority
Sleep is just as important as action and shouldn't be dependent on completing other tasks.
There are no specific guidelines that you have to follow, apart from the key principles for quality, restorative sleep that allows your body and mind to function properly.
Go to bed and get up at the same time every day. Create a sleep routine.
The bedroom should be cool, dark and quiet. Avoid screens before bed, at all costs. (Suggestion: Read a book about something you really like, and that makes you want to keep reading the next day)
If you can't fall asleep after 30 minutes of laying your head on the pillow, get up and do something quiet until you feel sleepy.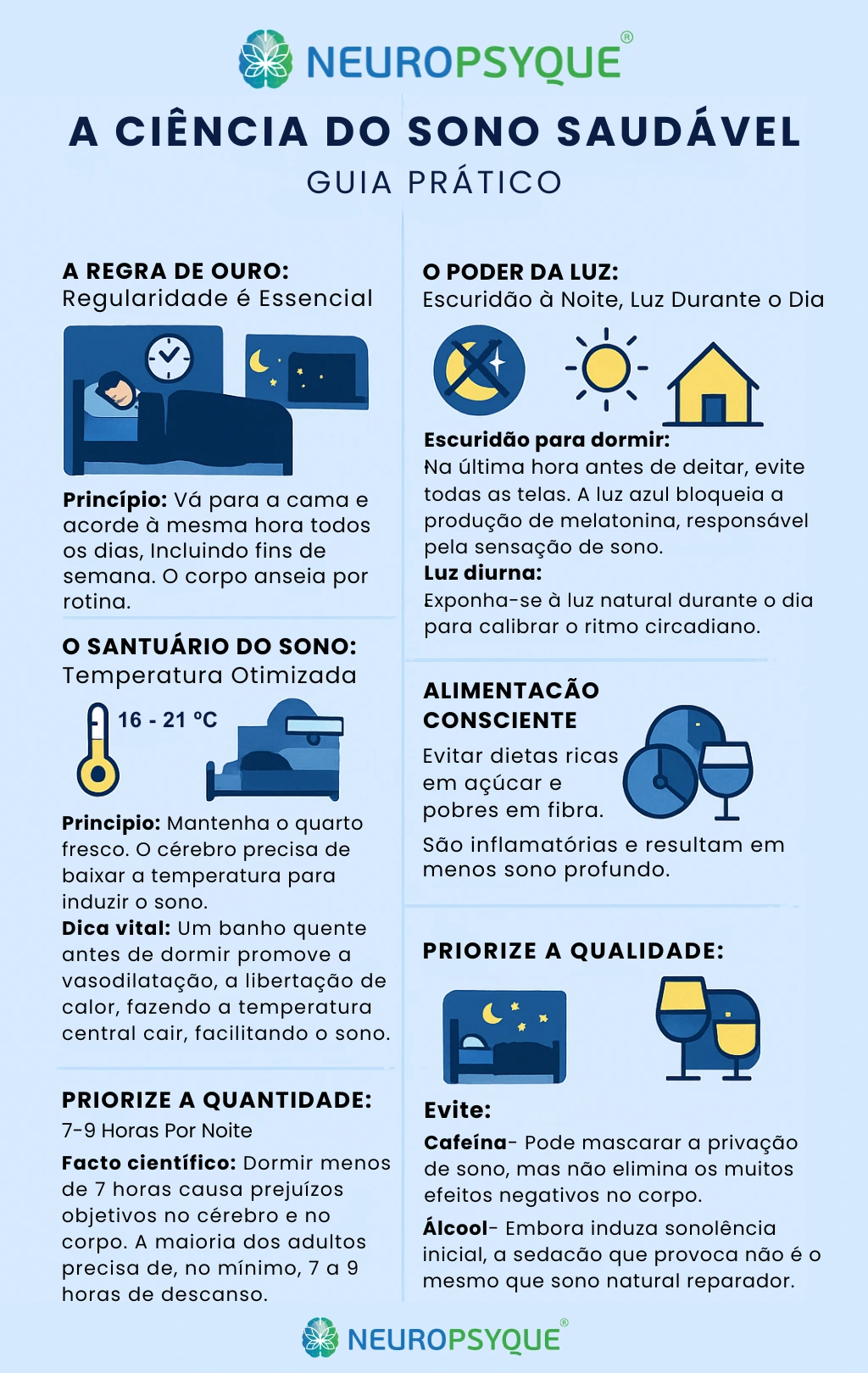
Social Connections
Depression feeds on isolation. Try to keep in touch with friends and family, even if it's brief messages, and even if it's difficult.
Take part in social activities, even for short periods. You don't have to stay for hours - 20 minutes is enough.
Be honest about your needs. "I'd like to go, but I can only stay for half an hour" is perfectly valid.
Be Kind to Yourself
Self-criticism is devastating. Talk to yourself as you would talk to a friend you admire.
First of all, recognise that nobody "is" depressed. Depression is a state, a temporary condition.
There are cases of chronic depression, with a strong neurological basis, in which some symptoms are very persistent and can last for decades, but in the vast majority of cases complete remission of many symptoms is achieved.
Myths and Truths about Depression
The stigma surrounding depression is still enormous. Many mistaken beliefs prevent many people from seeking help.
Let's dispel a few myths:
| ___MYTH___ | TRUTH |
| "Depression is just sadness" | Depression is a medical illness that affects the brain, body and behaviour. It's much more than sadness - it involves concrete and visible neurobiological changes. |
| "It's a lack of willpower" | Depression alters the structure and functioning of the brain. You can't overcome it with "positive thinking" or "willpower" alone, just as you can't cure diabetes with willpower alone. |
| "Antidepressants are always addictive" | Antidepressants don't create always addiction. Depressants and sedatives, including some antidepressants, are more likely to be addictive. Even so, there is always the possibility. |
| "People with depression are always sad" | Many people with depression feel more anhedonia (inability to feel pleasure), a kind of emptiness, than actual sadness. Some feel irritable, others show apathy. Sadness, however, is one of the most common symptoms. |
| "It will pass by itself" | Untreated depression rarely gets better on its own and can become chronic. Early diagnosis and timely treatment are key. |
| "It only affects fragile people" | Depression can affect anyone, regardless of strength of character, intelligence or social status. It's definitely not a sign of weakness. |
| "Talking about it makes it worse" | Talking to a qualified professional or someone you trust is an important part of recovery. Expressing your feelings helps, not hurts. However, there is great variability in the needs of different cases. In certain cases, the answer may be less about confronting the points of pain and suffering, and more about taking the focus off the causes of the pain. The two approaches can be used in the same treatment process, at different stages. |
| "If you can work, it's no big deal" | Many people with severe depression keep up appearances at work through immense effort, but suffer deeply. Often, it's when you're at your worst that you smile the most. This requires a lot of attention and should be studied by all of us. External functionality does not necessarily reflect internal suffering. |
| "There are people who ARE depressed" | No one is depressed by nature or endlessly. With appropriate treatment, many people recover completely and go on to lead normal lives. Even in recurrent cases, episodes can be prevented or managed effectively. Remember - 6 out of 10 Portuguese have experienced depressive symptoms. |
Fighting stigma is everyone's responsibility.
Depression is as real as diabetes, hypertension or any other chronic illness.
It's the disease MORE DISABLING worldwide, in numbers.
It deserves all seriousness and understanding.
Seeking treatment is a sign of courage and self-care, not weakness.
Recovery isn't just possible - it's common. Thousands of people recover every year.
Talking openly about mental health, and spreading knowledge about the condition, as this article seeks to do, is the key to reducing stigma and saving more lives.

Comorbidities Associated with Depression
Depression rarely occurs in isolation. It often coexists with other conditions.
Anxiety (25-50% of cases)
Depression and anxiety often overlap. Many people have both at the same time.
Here are some specific anxiety disorders that often coexist:
- Generalised Anxiety Disorder
- Panic Disorder
- Social Phobia
This is a combination that complicates health conditions and worsens the prognosis if left untreated. Fortunately, there are treatments that work for both.
Substance Abuse
Some people with depression turn to alcohol or the drugs in an attempt to self-medicate and look for temporary relief from suffering.
This creates a dangerous cycle.
This type of substance aggravates depression in the long term and complicates treatment. The bottom line, masks the pain but weakens habits and routine even moreThis helps to aggravate the symptoms.
In this case, treatment must address both problems simultaneously. Many people recover from both conditions.
Chronic Physical Diseases
The relationship between depression and physical illness is two-way.
What does this mean?
This means that depression is often caused and aggravated by physical illnesses, and physical illnesses are often enhanced by depression. Physical illness can cause depression, and depression can aggravate physical illness.
Here are some frequently associated conditions:
- Cardiovascular diseases - depression increases the risk of stroke
- Diabetes - management worse when there's depression
- Chronic pain and fibromyalgia - often lead to depression
- Autoimmune diseases - often lead to depression
- Cancer - often leads to depression
Other Psychological Disorders
Bipolar disorder
The depressive phases of the disorder can be confused with major depression. But the treatment is different - it's crucial to make the correct diagnosis.
Obsessive-Compulsive Disorder
It can coexist with depression. It often causes it.
Post-Traumatic Stress Disorder
Often accompanied by depression.
Eating Disorders
Anorexia, bulimia and depression often occur together.
Important differentiations
Depression vs. Normal Grief vs. Pathological Grief
A particularly difficult process of mourning, accompanied by symptoms typical of depression, is known in medicine as Prolonged Pathological Bereavement.
No Normal GriefThere are waves of sadness interspersed with positive memories of the lost person. The ability to experience moments of pleasure remains.
O Pathological Grief lasts for more than 12 months, and usually involves severe difficulty in accepting lossAlthough it contains some of the most characteristic symptoms of depression, such as anhedonia (generalised loss of interest).
For this reason, this condition deserves an independent diagnosis (DSM-5-TR).
Even though they have many symptoms in common, the approach to treatment is usually different.
Depression vs. Burnout
Burnout is increasingly common, and it is specifically work-related. There is professional burnout and decreased performance at work and in personal life.
Burnout has a brief treatment, dependent on specific lifestyle changes.
However, it can lead to depression - a rapid diagnosis is crucial.
Depression vs. Normal Sadness
Sadness is a feeling, an answer proportional to negative events. It gradually improves over time and does not seriously interfere with day-to-day functioning.
Depression is persistent beyond belief and significantly interferes with everyday life.
The possible presence of all these comorbidities emphasises the importance of a thorough and professional assessment. It's not enough to treat just one aspect - the whole person needs to be considered.
In conditions withn Depression, it is more important for the doctor to know "the person who has the illness" than "the illness that the person has".
In NeuroPsyqueOur integrated approach between specialities allows precisely this: a complete overview and comprehensive treatment.
Resources and Support Available in Portugal
You'll never be alone. There are many resources available in Portugal to support cases of depression.
Free helplines
| Service | _Contact_ | Timetable |
| National Emergency Line | 112 | 24h/day |
| National Suicide Prevention and Psychological Support Line | 1441 | 24h/day |
| SNS 24 - Psychological Counselling | 808 24 24 24 (option 4) | 24h/day |
| SOS Friendly Voice | 213 544 545 | 912 802 669 | 963 524 660 | 800 209 899 | 15.30 - 00.30 |
| Friendly chat | 808 237 327 | 210 027 159 | 3pm - 10pm |
| Friendly Voices of Hope from Portugal (VOADES) | 222 030 707 | 4pm - 10pm |
| Friendship Phone Number | 222 080 707 | 4pm - 11pm |
| Voice of Support | 225 506 070 | 21h - 00h |
Support Associations
| Organisation | Description |
| ADEB - Association for the Support of Depressive and Bipolar Patients | Individualised psychosocial support, support groups, psychoeducational workshops, suicide prevention |
| APAV - Portuguese Association for Victim Support | Support for victims of crime, including psychological support |
| Order of Portuguese Psychologists | Mental health information and resources |
Conclusion
Depression is a condition, a state, and not part of the identity. It exists in several types, with different symptomatic groups and treatment approaches.
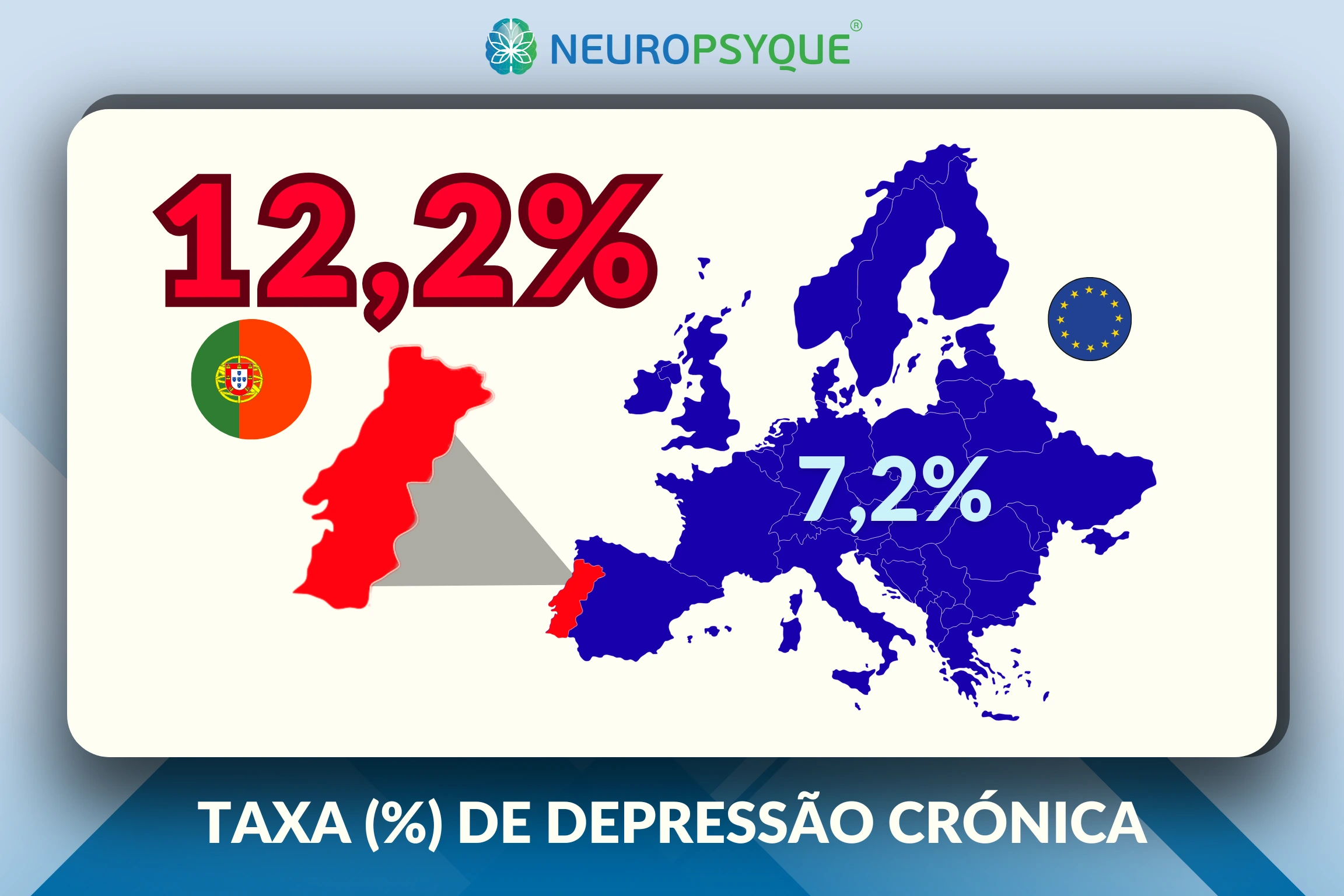
It is one of the most prevalent mental health conditions in Portugal. It is estimated that around 12% of the population suffers from chronic depression. More than 1 million cases, apart from all the cases of episodic depression, with even higher numbers.
The figures are worrying. Portugal leads the European Union in chronic depression. nº1.
But there is a fundamental message that needs to be echoed: depression is treatable.
A Transcranial Magnetic Stimulation represents hope. It is a transformative innovation, particularly for cases that are resistant to pharmacological treatment.
The integrated approach - combining different therapies thinking about the personand not just in eliminating symptoms - offers the best results.
The sooner you seek help, the better your prospects are. The average range of 5 years between symptoms and treatment in Portugal is far too long. Every day of avoidable suffering is one day too many.
Recovery is possible. It happens. Thousands of people recover from depression every year. With well-considered and appropriate treatment, you can feel good again. You can find meaning and pleasure in life again.
The road can be challenging. There will be better days and worse days. But you don't have to walk it alone.
If you recognise these symptoms in yourself or someone close to you, don't wait.
In NeuroPsyqueWe give our best, and the best that modern medicine has to offer.
Your life has unconditional value - fight for it and for those who need you.
↓ Leave us your questions - we'll be happy to answer them!
FAQ's about Depression
1. Can depression be cured?
Depression is treatable and many people recover completely. With appropriate treatment, around 60-75% of people experience significant improvement in symptoms. Some people have only one episode in their lives, others may have recurrences that require maintenance treatment. Even in recurrent cases, effective management allows for a full and satisfying life.
2. How long does it take to recover from depression?
It varies depending on the person and the severity of the depression. With treatment, many experience initial improvement in 2 to 4 weeks, but full recovery can take 3 to 6 months or more. More severe or long-term depression may require more time. Early treatment usually results in faster recovery. Improvement is gradual - small advances accumulate.
3. Can I treat depression without medication?
Yes, especially in mild to moderate cases. Cognitive Behavioural Psychotherapy is effective, and Transcranial Magnetic Stimulation is another extremely effective alternative to drugs. However, in moderate to severe cases, a combination of different treatments (psychotherapy, medication, neurotherapy) usually offers the best results. A professional specialising in the condition will help determine the best approach for your specific case.
4. Do antidepressants change my personality?
Usually not. If you feel that a medicine is changing your personality and having a negative effect on your mood and energy, you should tell your doctor - it may be necessary to adjust your dosage, change the drug or even stop treatment.
5. What if antidepressants don't work?
Around 30% of people have depression that is resistant to traditional pharmacological treatment. This doesn't mean that there is no solution. In these cases, Transcranial Magnetic Stimulation has proved particularly effective, with high response rates (58% post-pharmacological failure efficacy).
6. What is Transcranial Magnetic Stimulation for depression?
It's an internationally approved non-invasive technique that uses focused magnetic pulses to stimulate specific areas of the brain related to mood. It works by modulating neuronal activity and rebalancing neurotransmitters. It has level A scientific evidence (the highest rating) for the treatment of depression. It requires no anaesthetic and has the great benefit of having minimal side effects, allowing you to resume activities immediately after each session.
7. Can depression return after treatment?
There may be recurrences, especially in people with a history of multiple episodes. For this reason, maintenance treatment (ongoing psychotherapy, preventive medication, or both) may be recommended after recovery. Learning management strategies, recognising early warning signs, and maintaining healthy habits significantly reduces the risk of relapse. Regular follow-up with a specialist also helps to prevent or detect new episodes early on.
8. How can I help someone with depression?
Listen without judgement. Validate the person's feelings ("I understand that you're suffering"). Encourage them to seek professional help and offer your support and closeness. Be patient - recovery takes time. Avoid phrases like "cheer up", "there are people worse off" or "it's just willpower". Learning about the nature of the mind will always be useful.
9. Is depression hereditary?
There is a genetic component to depression. Having a close relative with depression increases the risk of diagnosis 2 to 3 times. However, genetics is not destiny. Many people with a family history never develop depression, and many people without a history do. Environmental, psychological and social factors are very important. Having a family member with depression means greater vigilance and attention to symptoms, not that you will inevitably develop the condition.
10. Does exercise really help with depression?
Yes, the evidence is strong. Regular exercise has a proven antidepressant effect, comparable to many drugs in some studies, and without the unwanted effects. 30 minutes a day of moderate activity (such as walking) is enough to reap the benefits. Exercise increases mood-related neurotransmitters, promotes neurogenesis (the creation of new neurons) and improves sleep and self-esteem. Starting with small steps is important - 5 minutes counts. The important thing is to incorporate physical activity into your life.
11. How long does the first consultation at NeuroPsyque take?
Our consultations are extended precisely to allow for a complete and in-depth understanding of the situation. The first consultation usually lasts between 60 and 90 minutes. This time allows the doctor to listen carefully to your story, make a detailed assessment, clarify any doubts and discuss the best personalised treatment plan together. We don't rush through appointments - your well-being deserves time and attention.
12. Why choose NeuroPsyque to treat my depression?
We offer a truly integrated approach between specialities (Neurology, Psychiatry, Neuropsychology, Physiotherapy and PNEI), and a treatment specifically moulded to you. We have state-of-the-art equipment, from EMT, à tDCS, to Neurofeedbacktherapies Physiotherapy, à Acupunctureamong other therapies. Our focus is on resolving causes, not just controlling symptoms - the improvement must be general and long-lasting. We work to give those who come to us the best possible expectation of improvement.
Medical Disclaimer:
This information is educational and does not replace professional medical advice. Depression should only be diagnosed and treated by qualified professionals (psychiatrists or clinical psychologists). If you have suicidal thoughts or are in crisis, contact 112, SNS 24 (808 24 24 24, option 4) or the 1411 helpline immediately. Your life has unconditional value and help is available.