In Portugal, it is estimated that more than 193,500 people live with dementiaand Alzheimer's disease represents between 50 and 70% of these cases. Portugal ranks 4th place among the OECD countries with the highest prevalence per thousand inhabitants, with 19.9 cases compared to the average of 14.8. By 2037, projections point to 322,000 cases. But is Alzheimer's just an inevitable consequence of ageing?
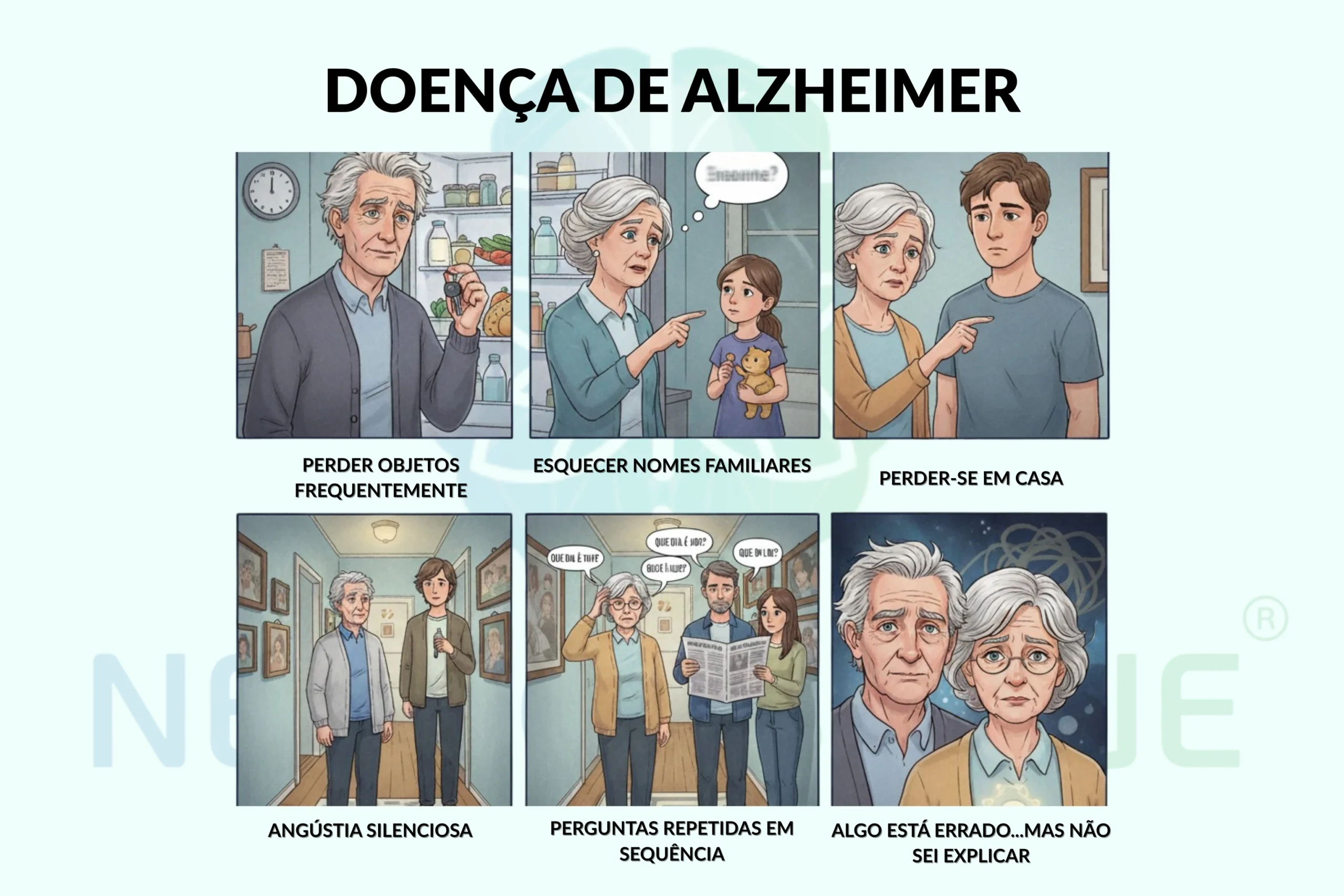
It's looking for your keys for 10 minutes and finding them in the fridge. It's forgetting the name of the grandchild you visited yesterday. It's feeling lost in the very house you've lived in for 30 years. It's seeing frustration in the family's eyes when he asks for the fifth time, "What day is it?" It's the silent anguish of knowing that something is wrongbut he couldn't explain exactly what.
For millions of Portuguese, including those who deal indirectly with the conditionthese are not just "memory lapses of age" - are the first signs of a reality that is completely transforming the way people live and relate to the world.
Alzheimer's disease it's not mental laziness, lack of effort or simply "ageing badly". It is a real neurological condition with specific changes in the brainIn many cases, this can be identified, treated and, in many cases, its progress can be significantly slowed down.
What is Alzheimer's Disease?
Alzheimer's disease is a progressive neurodegenerative disorder, and is the most common form of dementia. It is characterised by the progressive death of brain cells (neurons) and the abnormal accumulation of proteins in the brain, leading to gradual and irreversible deterioration of cognitive, behavioural and functional functions.
Contrary to what many people think, Alzheimer's is not a natural consequence of ageing. It is a specific disease that affects particular regions of the brain, usually starting with the hippocampus (area responsible for memory) and progressively spreading to other areas of the brain.
Medical Definition
A World Health Organisation classifies Alzheimer's disease in the ICD-11 as a neurodegenerative dementia characterised by two main types of brain damage:
- Senile plaques: Deposits of beta-amyloid protein that accumulate around neurons
- Neurofibrillary braidsIntracellular accumulations (within neurons) of hyperphosphorylated tau protein
Recognition in Portugal
In Portugal, Alzheimer's disease is officially recognised by the National Health System as an chronic condition that requires specialised multidisciplinary monitoring. However, recent studies of the Institute of Public Health of the University of Porto revealed a national peculiarity: unlike other Western countries, vascular dementia (resulting from damage to the circulatory system) is more prevalent than Alzheimer's in Portugaloften resulting from complications of strokes.
Difference Between Alzheimer's and Normal Forgetfulness
It is essential to distinguish between the natural forgetfulness of ageing and the initial symptoms of Alzheimer's disease.
| Features | Normal forgetfulness | Alzheimer's disease |
| Type of memory affected | Occasional details | Complete recent events |
| Frequency | Sporadic | Consistent and progressive |
| Functional impact | Minimum | Interferes with daily activities |
| Guidance | Maintained | Temporal and spatial confusion |
| Recognising the problem | Aware of lapses | Often denies or doesn't realise |
| Ability to remember with clues | Can remember with help | It doesn't get any better with trails |
| Progression | Stable over time | Continuous deterioration |
Practical examples
Normal forgetfulness:
- Forgetting where you put your glasses but finding them after searching
- Not remembering the name of a distant acquaintance
- Hesitating on a word during a conversation
Signs of Alzheimer's:
- Forgetting entire conversations you had yesterday
- Not recognising close family members
- Getting lost in familiar places
- Placing objects in unusual places (keys in the fridge)

Most common symptoms of Alzheimer's
The symptoms of Alzheimer's disease manifest themselves in the following ways progressive and can vary between individuals, but follow recognisable patterns.
Initial Symptoms (First manifestation)
The first and most characteristic symptom is recent memory loss. This includes:
- Forgetting recently learnt information
- Repeat the same questions
- Need constant reminders for routine tasks
- Difficulty remembering important dates and events
Progressive Cognitive Symptoms
As the disease progresses, other symptoms emerge:
- Language difficultiesProblems finding words, following conversations or naming common objects
- Spatial and temporal disorientationGetting lost in familiar places, confusion about the day, month or year
- Thinking problemsDifficulty solving problems, doing simple calculations or planning activities
- Changes to the judgementInappropriate decisions about money, personal care or security
Behavioural and Psychological Symptoms
- Personality and mood swings
- Irritability, aggression or apathy
- Anxiety or depression
- Paranoia or unjustified mistrust
- Sleep disturbances
- Tendency to social isolation
Variations by Age
Early onset Alzheimer's (before the age of 65):
- Often faster progression
- Largest genetic component
- Symptoms may be less typical initially
Late-onset Alzheimer's (after 65 years):
- Most common (accounts for 95% of cases)
- Evolution usually slower
- Symptoms follow a more predictable pattern

Stages of Alzheimer's Disease
Alzheimer's disease progresses through different phasesalthough the speed and duration can vary significantly from person to person.
Early/Little phase (2-4 years)
At this stage, the person still maintains some independencebut the symptoms become apparent to close family members:
- More pronounced recent memory loss
- Slight difficulties with complex tasks (financial management, cooking)
- Subtle language problems
- Slight changes in personality
- Temporal disorientation begins
The person can still live alone, but needs occasional supervision.
Moderate Phase (2-10 years)
It's typically the longest phase and when the need for care becomes apparent:
- Significant memory loss, including past events
- Difficulty recognising familiar people
- Need for help with daily activities (dressing, washing, eating)
- Marked spatial disorientation
- Most obvious behavioural changes
- More severe communication problems
- Onset of motor problems
Severe/Terminal Phase (1-3 years)
In this final phase, the person becomes totally dependent:
- Almost complete loss of ability to communicate
- Urinary and faecal incontinence
- Difficulty swallowing
- Loss of mobility
- Increased susceptibility to infections
- Need 24-hour care
Causes and risk factors
Alzheimer's disease results from a complex interaction between multiple factorsThere is no single identifiable cause.
Genetic factors
Familial Alzheimer's (5% of cases):
- Mutations in the APP, PSEN1 and PSEN2 genes
- Usually starts before the age of 65
- Risk of 50% for children if one parent is a carrier
Main Genetic Risk Factor:
- APOE4 gene: Increases risk by 3-4 times
- Two copies of APOE4: 95% carriers develop brain changes by the age of 82
- Present in around 25% of the Portuguese population
Neurobiological factors
Characteristic brain changes include
- Beta-amyloid plaques: Accumulation of toxic protein between neurons
- Tau protein braids: Aggregates inside neurons that prevent normal functioning
- Brain inflammation: Immune response that can aggravate the damage
- Loss of synaptic connectionsReduced communication between neurons
Modifiable Risk Factors
These factors can be controlled through lifestyle changes:
- Cardiovascular factors: Hypertension, diabetes, high cholesterol, obesity
- LifestyleSedentary lifestyle, smoking, excessive alcohol consumption
- Social factors: Social isolation, low schooling, lack of cognitive stimulation
- Mental health: Untreated depression, chronic stress
Non-Modifiable Risk Factors
- AgeMain risk factor (doubles every 5 years after the age of 65)
- Gender: Women have a higher risk, possibly due to their greater longevity
- Family history: Increases risk even in the absence of specific mutations
- Head traumaEspecially if repeated or severe
Diagnosing Alzheimer's
The diagnosis of Alzheimer's disease is fundamentally clinicalThis is based on a detailed medical assessment that includes a clinical history, neurological examination, cognitive tests and complementary examinations.
Complete Diagnostic Process
Diagnosis follows several essential stages:
- Detailed medical history with the patient and family
- Cognitive assessment through standardised tests
- Physical and neurological examination complete
- Complementary tests to exclude other causes
- Time tracking to observe the evolution
Updated diagnostic criteria
The current criteria are based on the Alzheimer's Association International and follow a biomarker approach:
Main Criteria:
- Cognitive decline in relation to previous functioning
- Significant interference in daily activities
- Exclusion of other causes of dementia
- Progressive development of symptoms
Main Neuropsychological Tests:
Mini Mental State Examination (MMSE)
- Assesses orientation, memory, attention, calculation and language
- Maximum score: 30 points
- Suspected dementia: < 24 points (adjusted for education)
Montreal Cognitive Assessment (MoCA)
- More sensitive to slight changes
- Evaluates multiple cognitive domains
- Better for early detection
New blood tests for early detection
Ongoing a revolution in diagnostics with the development of blood biomarkers.
PrecivityAD2 test:
- Analyses the proportion (ratio) of beta-amyloid proteins (42/40) and tau p217
- Accuracy of 90-95% compared to other tests
- Less invasive than lumbar puncture or brain PET scan
Advantages of Blood Tests:
- Detection up to 20 years before symptoms
- Easier access to primary care
- Lower cost
- Enable earlier diagnosis and timely treatment
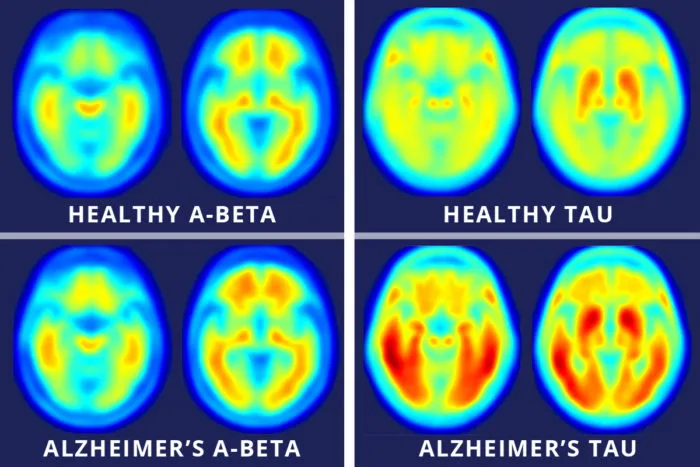
Brain PET scan:
- PET-amyloid: Detects beta-amyloid plaques in the brain
- PET-tau: Visualises tau protein distribution
- High diagnostic accuracy but high cost
Importance of Early Diagnosis
O early diagnosis allows:
- Timely initiation of effective treatments
- Better family and financial planning
- Access to clinical trials of new treatments
- Implementation of secondary prevention strategies
Impact of Alzheimer's on daily life
Alzheimer's profoundly affects not only the person diagnosed, but their entire family and social circle.
Patient Impact
Progressive loss of autonomy:
- Increasing inability to perform basic activities (washing, dressing, eating)
- Difficulties in managing finances and medication
- Loss of ability to drive
- Progressive social isolation
Emotional impact:
- Frustration at the loss of skills
- Anxiety about the uncertain future
- Depression (present in 40-50% of cases)
- Loss of identity and self-esteem
Family Impact
Carers' stress:
- 75% of family carers develop significant stress
- Increased risk of depression and anxiety
- Carers' own social isolation
- Impact on marital and family relationships
Financial charges:
- Direct treatment and care costs
- Loss of family income
- Need for housing adaptations
- Possible need for residential care
Social and Economic Impact
For society:
- Costs estimated at 604 billion dollars worldwide
- Pressure on health and social security systems
- Growing need for specialised professionals
- Impact on the workforce (family carers)
Mortality Rate and Prognosis
Alzheimer's disease has a variable prognosis:
- Life expectancy after diagnosis: 4-8 years on average
- It can extend to 20 years in some cases
- Main cause of death: respiratory infections, not the disease itself
- Indirect mortality due to progressive disability

How is Alzheimer's treated?
Although there is still no definitive cure for Alzheimer's disease, multiple therapeutic approaches can significantly slow progression and improve quality of life.
Treatment should always be multidisciplinary and personalisedIt combines different strategies based on the stage of the disease and the individual needs of each patient.
Medicines used for treatment
The vast majority of drugs used to treat Alzheimer's increase levels of acetylcholine, a neurotransmitter that is crucial for memory.
Donepezil (Aricept)
- Effective at all stages of the disease
- Dose: 5-10mg per day
- Recently approved by SUS for severe stages
- Can be combined with memantine
Rivastigmine (Exelon)
- For mild to moderate phases
- Available as tablets or transdermal patches
- Patches reduce gastrointestinal effects
Galantamine (Reminyl)
- For mild to moderate phases
- Dual action: inhibits cholinesterase and modulates nicotinic receptors
- Prolonged-release tablets
Memantine
- Mechanism: Regulates glutamate activity
- Indication: Moderate to severe stages
- Benefits: May delay functional deterioration
- Combination: Often used with cholinesterase inhibitors
Lecanemab (Leqembi)
- Approved by EMA in 2024
- Reduces 27% cognitive progression in studies
- Demonstrates effective removal of amyloid plaques
- High cost: ~130,000 euros/year
Neurotherapy - Transcranial Magnetic Stimulation (TMS)
Neurotherapy represents one of the most promising and innovative approaches to treating Alzheimer's, offering an effective and safe alternative with growing scientific evidence.
EMT is a non-invasive technique that uses magnetic fields to modulate brain activity in specific regions:
How it works:
- Magnetic pulses directed at the dorsolateral prefrontal cortex
- High frequency (10Hz) during 20-30 typical sessions
- Stimulates neuroplasticity and improves neural connections
- Acts on memory circuits, attention and executive functions
Proven benefits:
- Significant improvement in memory and cognitive functions
- Reduction of associated depressive symptoms
- Stabilisation of the clinical picture for 6+ months
- Increased quality of life for patient and family
Scientific evidence:
- Multiple controlled studies show efficacy
- Improvement maintained in long-term follow-up
- Established safety with minimal side effects
Advantages of Neurotherapy:
Compared to traditional pharmacological treatments, Neurotherapy offers:
- Superior safety profile: No significant systemic side effects
- No dependency: No risk of tolerance or withdrawal syndrome
- Lasting benefits: Effects continue months after treatment
- ComplementaryCan be combined with medication
- Personalisation: Adapted to individual brain patterns
Complementary therapies
Cognitive stimulation
Structured programmes to exercise mental functions:
- Memory and attention exercises
- Cognitive games adapted to functional level
- Reminiscence therapy
- Multi-sensory stimulation activities
Cognitive Behavioural Therapy
- Behavioural symptom management
- Reduced anxiety and depression
- Adaptation strategies for patient and family
- Improved quality of life
Physical Activity and Physiotherapy
- Regular aerobic exercise reduces the risk of progression
- Maintaining mobility and balance
- Reduced risk of falls
- Cardiovascular benefits that protect the brain
In NeuroPsyque our commitment is, as always, to provide you with the greatest possible expectation of improvement.
We have the most specialised equipment and experts in areas such as Neurology and Neuropsychologyand also in therapies such as Transcranial Magnetic Stimulationwhich has proved important in the treatment of Alzheimer's. Book your appointment with us!

When to seek professional help
It is essential to look for specialised assessment when they identify persistent signs which may indicate the onset of Alzheimer's disease.
Specific warning signs
Seek medical help if you notice:
- Memory loss that interferes with daily life (not just occasional forgetfulness)
- Difficulty planning or solving problems that used to be easy
- Confusion with time or place - getting lost in familiar places
- Word problems when speaking or writing
- Placing objects in unusual places and I can't retrace my steps
- Decreased discernment - inappropriate financial decisions
- Changes in mood or personality - depression, anxiety, mistrust
When it's Urgent
Seek medical help immediate identify yourself:
- Sudden and severe disorientation
- Dangerous behaviour (leaving the gas open, dangerous driving)
- Hallucinations or delusions
- Uncontrolled aggression
- Suicidal ideation or self-injury
- Sudden inability to recognise close relatives
Importance of Early Intervention
Diagnosis and treatment early can:
- Significantly slow the progression of the disease
- Preserving functional capacities for longer
- Improve the quality of life of the patient and family
- Allow for better family planning and preparation
- Increasing the effectiveness of available treatments
How to deal with Alzheimer's in everyday life?
In addition to specialised medical care, there are essential practical strategies to improve the quality of life of both patients and carers.
Strategies for Family Members
Effective communication:
- Speak clearly and slowly
- Use simple, direct sentences
- Maintain eye contact
- Be patient and allow time for answers
- Avoid constant correcting or arguing
Maintaining dignity:
- Include the person in decisions whenever possible
- Respect their preferences and habits
- Valuing the skills you still have
- Avoid talking about the person as if they weren't there
Environmental adaptations
Housing security:
- Remove loose carpets and obstacles
- Install handrails and grab rails
- Improve lighting, especially at night
- Hiding dangerous objects (knives, medicines)
- Consider special locks to prevent leaks
Organisation of space:
- Maintain consistent routines and locations
- Labelling cupboards and drawers with pictures
- Wearing large calendars and watches
- Create calm spaces for relaxation
- Reduce noise and visual clutter
Hygiene and safety precautions
Personal hygiene:
- Simplify bathing and dressing routines
- Wear clothes that are easy to put on (Velcro instead of buttons)
- Establish regular schedules
- Prepare everything in advance
- Respect modesty and privacy
Food:
- Offer regular, nutritious meals
- Adapt consistency according to swallowing capacity
- Supervise to prevent choking
- Use adapted utensils if necessary
- Maintain a calm environment during meals
Support for carers
Caring for a family member with Alzheimer's is extremely demanding:
Essential self-care:
- Maintaining your own physical and mental health
- Seek psychological support when necessary
- Sharing responsibilities with other family members
- Use home support services
- Consider day centres for temporary relief
Support resources:
- Support groups for family members
- Training in care techniques
- Specialised psychological support
- Family breathing services
Advances in scientific research
Alzheimer's research is in constant evolutionbringing renewed hopes for patients and families.
Recent Genetic Discoveries
International Study 2024
A study of more than 72,000 participants identified new genetic variants associated with Alzheimer's, confirming that:
- The disease has both psychiatric and metabolic components
- Multiple genes contribute to the risk
- Environmental factors can activate or deactivate risk genes
APOE4 Gene as a Genetic Form
Research from 2024 suggests that having two copies of the APOE4 gene should be considered a genetic form of the disease, not just a risk factor, since 95% of people with this configuration develop brain changes.
New Biomarkers
Proteins in the Blood:
- Tau p217: Most promising biomarker
- 42/40 amyloid ratio: Indicates brain accumulation
- Neurofilaments: Markers of neuronal damage
- GFAP: Indicates glial activation and inflammation
Future prospects
Personalised Medicine:
- Treatments based on genetic profile individual
- Therapies aimed at specific subtypes of the disease
- Targeted prevention in high-risk individuals
Therapies in Development:
- Anti-tau" antibodies to treat neurofibrillary braids
- Modulators of cerebral inflammation
- Stem cell therapies
- Deep brain stimulation for selected cases
Advanced Immunotherapy:
- Vaccines against pathological proteins
- Safer new generation antibodies
- Targeted combination therapies

Myths and Truths about Alzheimer's
Clearing up misconceptions is fundamental to reduce stigma and promote a proper understanding of the disease.
| Myth | Truth |
| "Alzheimer's is a natural consequence of ageing" | Alzheimer's is a specific disease, not a normal ageing process. Many people reach the age of 90+ with no signs of dementia. |
| "Alzheimer's is always hereditary" | Only 5% of cases are hereditary. The majority result from an interaction between multiple genetic and environmental factors. |
| "Alzheimer's has no treatment" | There are multiple therapeutic options that can slow down progression and significantly improve quality of life. |
| "Alzheimer's only affects memory" | The disease affects multiple functions: language, reasoning, orientation, personality, behaviour and motor skills. |
| "It's impossible to prevent Alzheimer's" | Lifestyle factors such as exercise, a Mediterranean diet, cognitive stimulation and cardiovascular control can significantly reduce the risk. |
| "People with Alzheimer's don't understand what's going on" | Especially in the early stages, many people remain aware of their condition and can participate in decisions about care. |
| "Alzheimer's only affects very old people" | Although it is more common after the age of 65, early-onset Alzheimer's can affect people aged 30-50, especially with a genetic component. |
Resources and support available in Portugal
Portugal has several resources and organisations dedicated to supporting people with Alzheimer's and their families.
| Resource | Description | Contact |
| Alzheimer Portugal | National support association for relatives and patients. Information, training and psychosocial support | 963 604 626 |
| National Health Service | Neurology, psychiatry and neuropsychology consultations through the family doctor | Family doctor |
| SNS 24 line | 24-hour telephone support for health issues | 808 24 24 24 |
| University Hospitals | Specialised consultations in dementia and cognitive neurology | Several central hospitals |
| Specialised Day Centres | Cognitive stimulation and support during the day to relieve carers | Available regionally |
| SCML - Misericórdia de Lisboa | Residential care and specialised home support | 213 235 200 |
Specific support in Portugal
Medication through the NHS:
- Donepezil, rivastigmine, galantamine and memantine available free of charge
- Access through the Specialised Component of Pharmaceutical Assistance (CEAF)
- Application form (LME) completed by a specialist required
Rights and Social Support:
- Possibility of assigning a degree of disability
- Dependency allowance for family carers
- Exemption from user charges
- Home support through health centres
Conclusion
Alzheimer's disease is a condition complex and challenging which affects millions of people around the world, including more than 100,000 Portuguese. Although there is still no definitive cure, it is essential to emphasise that there is real hope e increasingly effective treatments which can significantly transform the course of the disease.
Key points to remember:
O early diagnosis is crucial. New blood biomarkers and imaging techniques make it possible to identify the disease years before the first symptoms, opening up windows of opportunity for more effective interventions.
A Neurotherapy represents a revolution in treatment, offering safe and effective alternatives with solid scientific evidence. Techniques such as Transcranial Magnetic Stimulation have been shown to stabilise the clinical picture and improve quality of life without the side effects of traditional pharmacological treatments.
A scientific research is advancing rapidly, with new drugs such as Lecanemab showing promising results, and personalised medicine based on genetic profiles moving closer to clinical reality.
For families and carers, it is essential to understand that you're not alone. There are resources, support and treatments available in Portugal that can make a significant difference in the management of the disease.
A prevention through healthy lifestyles - regular exercise, a Mediterranean diet, cognitive stimulation, cardiovascular control - can substantially reduce the risk of developing the disease.
There is hope. Each person is unique, and finding the ideal therapeutic combination may take time and adjustments, but it's worth persevering. Alzheimer's is not a definitive judgement.
In NeuroPsyquewe work every day to give the best possible expectation of improvement for our patientsusing a truly integrated approach that combines the best of Neurology, Neuropsychology, e Advanced neurotherapy.
FAQ's about Alzheimer's
1. Is Alzheimer's hereditary?
Only 5% of cases are hereditary (familial Alzheimer's). The majority result from an interaction between genetic and environmental factors. Having family members with Alzheimer's increases the risk, but does not guarantee that you will develop the disease. The APOE4 gene increases the risk, but many people with this gene never develop Alzheimer's.
2. What is the difference between Alzheimer's and dementia?
Dementia is a general term describing symptoms of cognitive decline. Alzheimer's is a specific type of dementia, accounting for 50-70% of all cases. Other dementias include vascular dementia, dementia due to Lewy bodies and frontotemporal dementia.
3. How is the diagnosis made?
Diagnosis is based on clinical history, neurological examination, cognitive tests (such as MMSE) and complementary examinations. New blood tests such as PrecivityAD2 can detect biomarkers with 90-95% accuracy. MRI and PET brain scans complement the assessment.
4. Is there a cure for Alzheimer's?
There is still no definitive cure, but symptoms can be significantly controlled and progression slowed with appropriate treatments. New drugs show the ability to modify the course of the disease, reducing progression by up to 27%.
5. How long does the treatment take?
Treatment is continuous and lifelong. Medications can take 6-12 weeks to show an effect. Neurotherapy can show benefits after 10-20 sessions, with effects maintained for 6+ months. Early treatment maximises benefits.
6. Is neurotherapy effective for Alzheimer's?
Yes, multiple controlled studies have demonstrated the efficacy of Transcranial Magnetic Stimulation and Neurofeedback. These techniques can stabilise the clinical picture, improve cognitive functions and quality of life, with a higher safety profile than medication.
7. How can Alzheimer's be prevented?
Although it is not 100% preventable, you can significantly reduce the risk through: regular physical exercise, a Mediterranean diet, cognitive stimulation, blood pressure and diabetes control, not smoking, maintaining an active social life and managing stress.
8. What are the first symptoms?
The most common first symptom is recent memory loss - forgetting conversations, events or recently learnt information. Other early symptoms include difficulty finding words, temporal disorientation and problems with complex tasks.
9. Does exercise help?
Yes, substantially. Regular aerobic (cardiovascular) exercise can reduce the risk of developing Alzheimer's in 30-40% and delay progression in people already diagnosed. It benefits cerebral circulation, promotes neurogenesis (neuronal reproduction) and reduces inflammation.
10. How to support a family member with Alzheimer's?
Maintain consistent routines, communicate clearly and patiently, preserve the person's dignity, seek support for yourself, use available resources such as day centres, and consider specialised psychological support for the whole family.
11. Are there support groups in Portugal?
Yes, Alzheimer Portugal offers support groups for family members and carers in various regions. Many health centres and hospitals also offer support programmes. Call 963 604 626 for more information.
12. When should I seek a second opinion?
Seek a second opinion if: the diagnosis is unclear, there is no improvement with current treatment, you want to explore options such as Neurotherapy, or if progression seems unusually rapid. An accurate diagnosis and optimised treatment can make a big difference.