In Portugal, it is estimated that 0.4% of the population suffers from anorexia nervosa - about 4 out of 1000 people. Although it may seem a low percentage, it represents thousands of lives at risk, because anorexia nervosa has the highest mortality rate of all psychiatric disorders.
It's looking in the mirror and seeing a "fat" person when everyone around you says you're "just skin and bones". It's obsessively counting every calorie, turning family meals into silent battlefields, and feeling a strange relief when the scales show one less kilo. It's hearing your family say "just eat a little bit" as if it were that simple, when every bite feels like a betrayal of the control that has become the only thing you can master in a life that seems out of your control.
For those living with anorexia nervosa, it's not vanity, it's not "a phase" or "wanting to attract attention". It is a mental prison where the body becomes both enemy and hostage, where hunger becomes a habitual and familiar companion, and where losing weight is the only victory in a world that seems to demand constant perfection.

What is Anorexia?
Anorexia nervosa is a severe eating disorder characterised by extreme restriction of food intake, intense fear of gaining weight and distortion of body image. It's much more than "wanting to be thin" - it's a complex medical condition that profoundly affects physical, mental and social health.
Unlike a common diet, anorexia nervosa involves a fundamental change in the perception of one's own body and a dysfunctional relationship with food that is beyond conscious control. The person with anorexia sees themselves as overweight even when they are significantly below a healthy weight.
Medical Definition
According to DSM-5 (Diagnostic and Statistical Manual of Mental Disorders)Anorexia nervosa is characterised by three main criteria:
- Restricting energy intake which results in a significantly low weight
- Intense fear of gaining weight or behaviour that persistently interferes with weight gain
- Disturbed perception of body weight or shape or lack of recognition of the seriousness of the current low weight
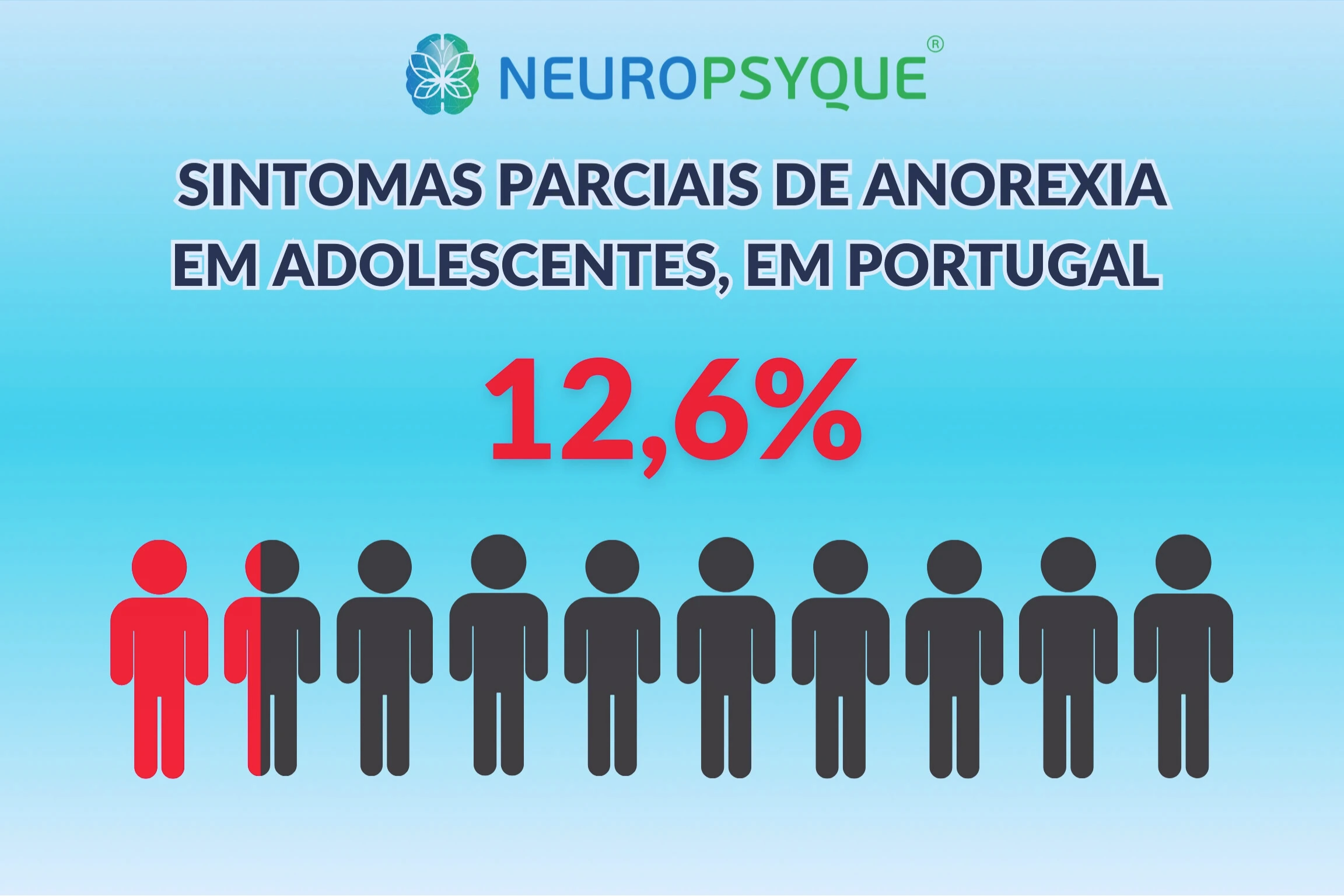
Recognition in Portugal
In Portugal, Anorexia Nervosa is officially recognised as a serious eating disorder. National data indicate that, although the prevalence is 0.3-0.4%, there are partial forms of the disease in approximately 12.6% of Portuguese adolescentsof the normal-weight girls reported a desire to lose weight, with 7% showing body image disturbance and 38% of the normal-weight girls reporting a desire to lose weight.
These figures deserve special attention, since anorexia nervosa has a mortality rate of between 10 and 20% of cases, and is the eating disorder with the highest mortality rate.
Difference Between Anorexia Nervosa and a Restrictive Diet
It is essential to realise that anorexia nervosa goes far beyond a normal restrictive diet. While a person on a diet seeks to lose weight in a controlled and healthy way, anorexia nervosa involves a pathological relationship with food and weight.
| Features | Normal Restrictive Diet | Anorexia Nervosa |
| Objective | Healthy weight loss | Total control through restriction |
| Body image | Realistic | Distorted (you see yourself as "fat" when you're thin) |
| Flexibility | Allows occasional exceptions | Rigid and inflexible rules |
| Social impact | Minimum | Isolation and family conflicts |
| Physical health | Maintained | Progressively compromised |
| Duration | Temporary | Persistent without treatment |
| Control | Volunteer | Compulsive, out of control |
The crucial difference is that in anorexia nervosa, food restriction becomes a compulsion that the person can't stop even when you rationally recognise that you need to eat.

Most common symptoms of anorexia
Physical symptoms
- Rapid and significant weight loss (more than 15% underweight)
- Extreme fatigue and constant weakness
- Amenorrhoea (absence of menstruation) or menstrual irregularities
- Hypotension and bradycardia (slow heartbeat)
- Extreme sensitivity to cold and always cold hands/feet
- Dry skin and the appearance of fine fluff on the body (lanugo)
- Hair loss and brittle nails
- Dizziness and frequent fainting
- Constipation chronic (bowels don't work)
- Concentration problems and "mental fog"
Psychological symptoms
- Obsessive worry with weight, calories and food
- Intense fear of gaining weight or putting on weight
- Distortion of body image (seeing yourself as "fat" when you're thin)
- Extreme perfectionism in various areas of life
- Low self-esteem linked to weight and appearance
- High anxietyespecially related to meals
- Depressive symptoms and irritability
- Denial of gravity weight loss
Behavioural symptoms
- Severe food restriction or elimination of food groups
- Obsessive calorie counting and frequent weighing
- Excessive physical exercise even though I'm weak
- Avoid social situations involving food
- Food rituals (cutting food into very small pieces, eating very slowly)
- Lying about the quantity of food consumed
- Wear loose clothing to hide weight loss
- Social isolation progressive
Variations by Age
Children (pre-adolescence):
- Stagnant growth or weight loss
- Sudden and persistent refusal to eat
- Concerns about "belly" or "fat"
Teenagers:
- Typical onset between the ages of 14-17
- Social pressure and comparison with peers
- Intense family conflicts over food
Adults:
- More subtle manifestations initially
- Greater ability to hide symptoms
- Often associated with stressful life events
Types of Anorexia
O DSM-5 identifies two main subtypes of anorexia nervosa, based on behaviour during the last 3 months:
Restrictive Type
In this subtype, the person doesn't get involved regularly episodes of compulsive eating or purging behaviour (self-induced vomiting, laxatives, diuretics).
Main features:
- Severe and controlled food restriction
- May involve excessive physical exercise
- Tendency towards greater control and rigidity
- Often associated with obsessive-compulsive traits
- They account for around 85-90% of cases
Purgative type
In this subtype, the person gets involved regularly in episodes of compulsive eating and/or purging behaviour.
Main features:
- Episodes of loss of food control followed by intense guilt
- Self-induced vomiting or use of laxatives/diuretics
- Greater impulsiveness compared to the restrictive type
- More obvious weight fluctuations
- Higher risk of acute medical complications
Causes and risk factors
Genetic factors
The research shows that strong hereditary component in anorexia nervosa. Even so, it's important to note that the transmitted tendency is not exclusively explained by genetic transmissionbut by behavioural factors associated with experience and the environment.
- Heredity of around 50-74% according to twin studies
- 6-10 times greater risk first-degree relatives
- Identification of 8 genetic variants associated with anorexia nervosa
- Recent genetic studies reveal that anorexia has both psychiatric and metabolic components
A 2019 international study published in Nature Genetics analysed data from more than 72,000 individuals and confirmed that anorexia nervosa has genetic correlations with disorders such as obsessive-compulsive disorder, major depression, anxiety and schizophrenia.
Psychological factors
- Extreme perfectionism and unrealistically high personal standards
- Low self-esteem and the need for external approval
- Difficulties in emotional regulation and inadequate coping strategies
- Obsessive-compulsive traits and the need for control
- Alexithymia (difficulty identifying and expressing emotions)
- Trauma or abuse (present in up to 50% of hospitalised cases)
Socio-cultural factors
- Social pressure to be thin and unattainable ideals of beauty
- Media influence and social networks
- Professional pressure (models, dancers, athletes...)
- Bullying or comments about weight or appearance
- Life transitions stressful events (change of school, parents' divorce...)
Neurobiological factors
Changes in neurotransmitter systemsin particular:
- Serotonin: Mood regulation and eating behaviour
- Dopamine: Reward and motivation system
- Noradrenaline: Appetite and weight regulation
- Changes in the prefrontal cortex related to executive control and decision-making

Diagnosing Anorexia
The diagnosis of anorexia nervosa is fundamentally clinicalbased on careful assessment of symptoms, behaviours and functional impact. There are no specific tests that "diagnose" anorexia nervosaBut various tests can support the diagnosis and assess complications.
Updated diagnostic criteria
For a diagnosis of anorexia nervosa, the following criteria must be present:
Criterion A - Energy Restriction: Restricted energy intake relative to needs, leading to significantly low body weight in the context of age, gender, developmental trajectory and physical health.
Criterion B - Intense Fear: Intense fear of gaining weight or putting on weight, or persistent behaviour that interferes with weight gain, even if they are significantly underweight.
Criterion C - Image disturbance: Disturbance in the way body weight or shape is experienced, undue influence of body weight or shape on self-evaluation, or persistent denial of the seriousness of current low body weight.
Severity Specifiers (based on BMI in adults)
The groups below indicate the severity of underweight using the Body Mass Index. BMI is calculated as follows:
BMI= weight(kg) / [height(cm) x height(cm)]. You can calculate your BMI here.
- Light: BMI ≥ 17 kg/m²
- Moderate: BMI 16-16.99 kg/m²
- Serious: BMI 15-15.99 kg/m²
- Extreme: BMI < 15 kg/m²
Diagnostic Process
Diagnosis involves several stages:
1. Detailed Clinical Assessment:
- Full medical and psychiatric history
- Assessment of current and historical eating patterns
- Exploring attitudes towards weight and body shape
- Assessment of psychosocial functioning
2. Physical examination:
- Weight and height measurement and BMI calculation
- Vital signs (blood pressure, heart rate)
- Assessment of signs of malnutrition
- General examination to identify medical complications
3. Complementary examinations:
- Full blood count
- Biochemical analyses (electrolytes, kidney function, liver function)
- Electrocardiogram
- Bone densitometry (if indicated)
4. Psychological assessment:
- Standardised questionnaires (EAT-26, EDI-3)
- Assessment of psychiatric comorbidities
- Analysing family and social support

The impact of anorexia on daily life
Anorexia nervosa profoundly affects multiple dimensions of lifecausing devastating consequences that extend far beyond weight loss.
Physical Impact
Cardiovascular System:
- Bradycardia (slow heartbeat, <60 bpm)
- Hypotension and risk of fainting
- Cardiac arrhythmias potentially fatal
- Reduced cardiac muscle mass
Bone System:
- Early osteopenia and osteoporosis
- Increased risk of fractures
- Growth retardation in adolescents
- Loss of bone density irreversible
Endocrine System:
- Amenorrhoea and infertility potentially irreversible
- Low oestrogen/testosterone levels
- Thyroid dysfunction
- Changes in cortisol
Digestive System:
- Gastroparesis (slow gastric emptying)
- Chronic constipation
- Atrophy of the intestinal villi
Psychological Impact
- Major depression (present in 70-80% of cases)
- Anxiety disorders (60-70% of cases)
- Obsessive-compulsive disorder (25-35% of cases)
- Cognitive difficulties: problems with concentration, memory and decision-making
- Suicidal ideation (risk 18 times higher to the general population)
Social and Family Impact
- Social isolation progressive loss of friendships
- Family conflicts intense food-related
- Overburdened carers and family stress
- Social incomprehension and stigma associated with the condition
Academic and Professional Impact
- Declining academic performance due to concentration difficulties
- Absenteeism from school or work frequent
- Abandonment of activities and previously valued projects
- Career limitations due to hospitalisations and treatment
Mortality rate
Anorexia nervosa has the highest mortality rate of all psychiatric disorders:
- Mortality rate of 0.56% per year
- 10% mortality per decade among people seeking treatment
- 12 times higher the mortality of young women in the general population
- Main causes of death: cardiovascular complications, kidney failure and suicide
How is Anorexia treated?
The treatment of anorexia nervosa requires a multidisciplinary and personalised approach, combining medical, psychological and nutritional interventions. The aim it's not just about regaining weightbut also restoring a healthy relationship with food and the body.
Multidisciplinary Approach
Effective treatment involves different competencesand generally a multi-speciality team.
- Neuropsychiatrist/Psychiatrist/Pedopsychiatrist: Assessment and treatment of psychiatric comorbidities
- Endocrinologist: Hormone monitoring and rebalancing
- Clinical psychologist: Individual and family psychotherapy
- Nutritionist: Food re-education and nutritional planning
- (optional) Medical doctor: Monitoring and treatment of medical complications
Neurotherapy
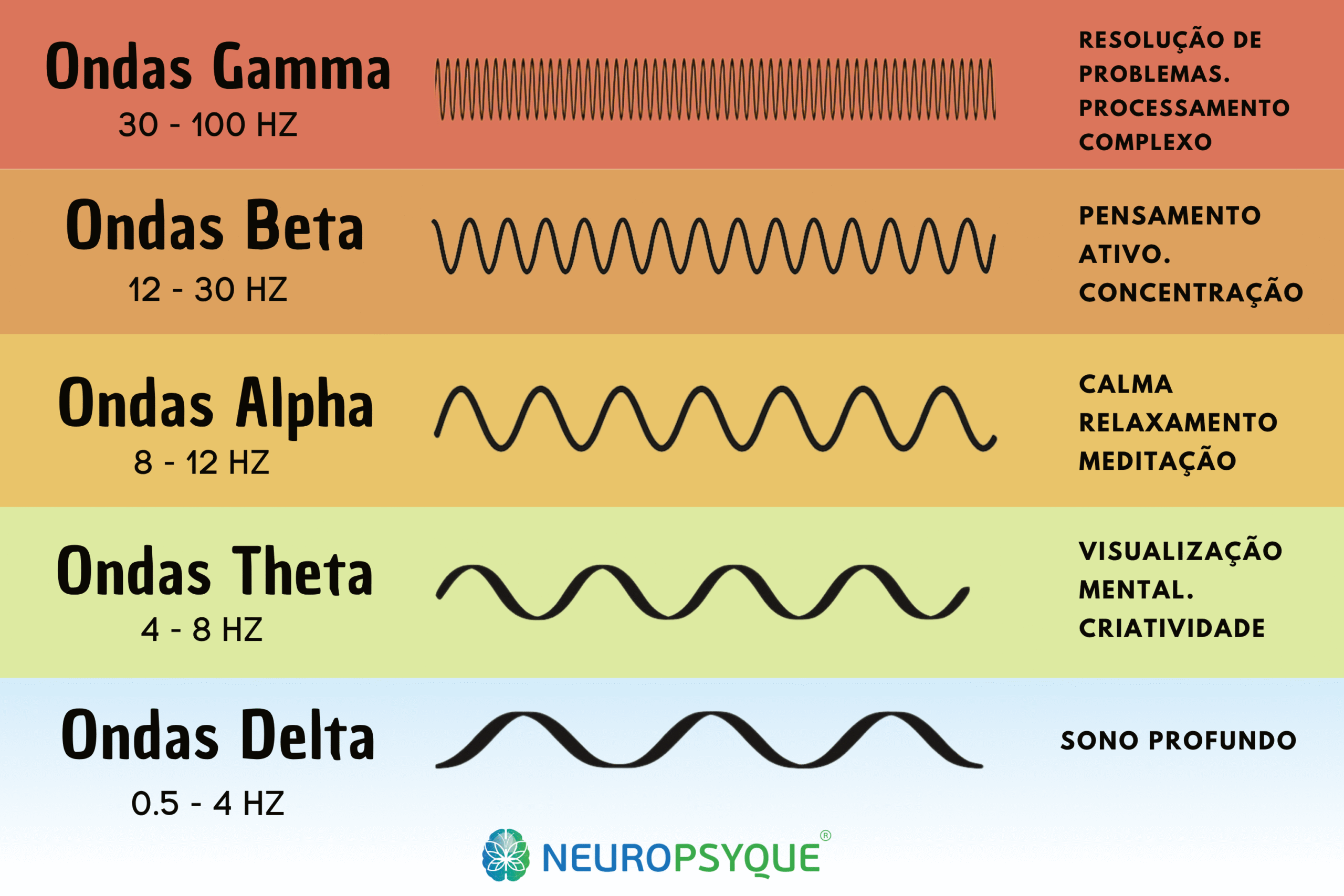
As we have seen, anorexia nervosa is associated with, and causes, neurological imbalances. Some of the most common imbalances are associated with neurotransmitters such as serotonin and noradrenaline.
As with many neuropsychiatric conditions, areas of the brain can be found in hyperactivity e hypoactivity (below normal), as well as significant changes in proportions in which the brain emits certain types of brain waves.
Neurotherapy makes it possible, in a precise way, correct these imbalancesand represents one of the most promising and innovative in the treatment of anorexia nervosa. It also presents a superior safety profile, with less risk of secondary damage, including addiction, compared to conventional pharmacological treatments.
Transcranial Magnetic Stimulation (TMS)
TMS currently represents a neuromodulation therapy with solid scientific evidence for anorexia nervosa, demonstrating effectiveness both in improving BMI and the central symptoms of the condition - PubMed CentralSpringer.
How it works:
- Modulates the dorsolateral prefrontal cortex (mainly left) involved in executive control
- Acts on brain circuits related to reward, decision-making and emotional regulation
- High frequency stimulation (10Hz) during 20-30 typical sessions
Documented benefits:
- Sustained weight gain - participants with a greater reduction in amygdala activity showed greater weight gain at 18 months - A pilot study exploring the effect of repetitive transcranial magnetic stimulation (rTMS) treatment on cerebral blood flow and its relation to clinical outcomes in severe enduring anorexia nervosa | Journal of Eating Disorders | Full Text
- Reducing the feeling of "feeling fat" and food-related anxiety - Repetitive transcranial magnetic stimulation treatment in severe, enduring anorexia nervosa: An open longer-term follow-up - PubMed
- Improved mood and associated depressive symptoms
- Proven safety and good tolerability in multiple studies - Repetitive Transcranial Magnetic Stimulation Strategies in the Treatment of Anorexia Nervosa: A Literature Review | American Journal of Psychiatry Residents' Journal
Advantages of EMT:
- Evidence of efficacy based on meta-analysis of 2025 - Efficacy of transcranial magnetic stimulation in anorexia nervosa: a systematic review and meta-analysis - PMC
- Non-invasive treatment with minimal side effects
- Can be combined with other therapies
- Results maintained in long-term follow-up
Disadvantages of EMT:
- It requires more investment, in the short termrather than just taking drugs
Transcranial Direct Current Stimulation (tDCS)
tDCS provides promising preliminary evidence for changing eating behaviour, while also maintaining minimal side effects - MDPIPubMed.
How it works:
- Modulates neuronal excitability through low-intensity electric current
- Anodic stimulation of the left dorsolateral prefrontal cortex
- Typical protocol: 2mA for 25-30 minutes per session
Documented benefits:
- Reduced need to follow specific dietary rules rigid - FrontiersPubMed
- Improved body image assessment in controlled studies - Frontiers | Effects of Transcranial Direct Current Stimulation Treatment for Anorexia Nervosa
- Reduction of depressive symptoms in some patients - Anodal transcranial direct current stimulation over the dorsolateral prefrontal cortex improves anorexia nervosa: A pilot study - PubMed
- Potential for change food intake patterns - The Effect of Transcranial Direct Current Stimulation (tDCS) on Anorexia Nervosa: A Narrative Review
Limitations:
- No significant effect weight gain in most studies (tDCS is used as a complement to other treatments, so it can be very effective) - Frontiers | Effects of Transcranial Direct Current Stimulation Treatment for Anorexia Nervosa

Specialised Psychotherapy
Cognitive Behavioural Therapy (CBT)
CBT is specifically adapted for anorexia nervosa:
- Identification and modification of dysfunctional thoughts about weight and eating
- Developing strategies to deal with food anxiety
- Cognitive restructuring body image distortion
- Relapse prevention through coping strategies
Family Therapy
Especially effective for teenagers and young adults:
- Maudsley model: Evidence-based family therapy
- Empowering parents to support nutritional recovery
- Improved family communication and conflict reduction
- 70-80% success rate in adolescents when started early
Third Generation Therapies
- Acceptance and Commitment Therapy (ACT): Focus on acceptance and personal values
- Compassion-Based Therapy: Development of self-compassion and self-esteem
- Mindfulness: Full awareness and emotional regulation
Pharmacological treatment
Drug treatment has significant limitations in anorexia nervosa:
Antidepressants:
- Limited effectiveness during the acute phase of low weight
- They can be useful after partial nutritional recovery
- Fluoxetine can help prevent relapses
Other drugs:
- Atypical antipsychotics (olanzapine) for extreme anxiety
- Nutritional supplements (calcium, vitamin D, multivitamins)
In NeuroPsyquewe offer a truly integrated approach that combines state-of-the-art neurotherapy with accompaniment neurological, psychiatric, neuropsychological, endocrine and nutritional specialisation. Our aim is to provide highest possible expectation of improvementusing the most advanced techniques available with a safety profile superior to conventional treatments.

When to seek professional help
It is essential to seek specialised assessment when signs of anorexia nervosa are identified. Early diagnosis and treatment are crucial for a favourable prognosis and the prevention of serious complications.
Don't wait for the condition to worsen.
Warning signs
Seek professional help if you notice:
- Significant weight loss (>15% of body weight) over a short period of time
- Persistent refusal to maintain normal weight for age and height
- Obsessive worry with weight, calories or physical appearance
- Avoidance of social situations involving food
- Excessive physical exercise even though she was visibly weak
- Lies about food or secretive behaviour
- Mood swings extremes related to weight or food
- Social isolation progressive
- Food rituals bizarre or inflexible
When it's Urgent
Seek immediate medical help if identified:
- Frequent fainting or severe dizziness
- Heart problems (irregular heartbeat, chest pain)
- Low body temperature persistent
- Severe dehydration or electrolyte imbalances
- Suicidal thoughts or behaviour
- Total refusal of food for prolonged periods
- BMI less than 15 or very rapid weight loss
Importance of Early Diagnosis
Early intervention in anorexia nervosa can:
- Prevent medical complications serious and irreversible
- Significantly improve prognosis (recovery rate >80% in adolescents)
- Reduce the duration and intensity of treatment required
- Minimising the impact physical and psychological development
- Prevent chronification condition
For Family and Friends
If you suspect someone close to you has anorexia nervosa:
- Approach the subject with compassion and without judgement
- Avoid comments about weight or appearance
- Offer support to seek professional help
- Educate yourself about the condition to better understand
- Make yourself available even if the person initially denies the problem
Advances in scientific research
Research into anorexia nervosa has advanced significantly in recent yearsThis has led to new insights into the causes of the condition and the development of more effective treatments.
Recent Genetic Discoveries
International Study 2019
A milestone in research was the study published in the journal Nature Genetics, which analysed data from more than 72,000 individuals from 17 countries:
Main findings:
- Identification of 8 genetic variants associated with anorexia nervosa
- Confirmation that anorexia nervosa has both psychiatric and metabolic components
- Genetic correlations with obsessive-compulsive disorder, depression, anxiety and schizophrenia
- Metabolic traits may be present before the disease develops
Implications for Treatment
These findings suggest that anorexia nervosa should be seen as a psychiatric and metabolic diseaseThis has important implications for the development of treatments:
- Targeted therapies based on the individual's genetic profile
- Metabolic approaches complementary to psychological treatment
- Possibility of early identification of individuals at risk
- Drug development more specific and effective
Emerging Treatments
Digital Medicine
- Mobile applications based on CBT for ongoing support
- Virtual reality for gradual exposure to food situations
- Artificial intelligence for monitoring behavioural patterns
- Telemedicine for specialised remote monitoring
Innovative Therapies
- Therapy based on neuroplasticity for brain restructuring
- Intestinal microbiota and its relationship with eating behaviour
- Psilocybin therapy (under experimental investigation)
- Deep brain stimulation for extremely resistant cases
Future prospects
Precision Medicine
The next few years promise to revolutionise the treatment of anorexia nervosa:
- Personalised treatments based on genetic and neurobiological profiling
- Biomarkers to predict response to treatment
- Targeted prevention in high-risk individuals
- Combined therapies optimised for each patient
Ongoing research
- Longitudinal studies to better understand the evolution of the disease
- Family research on transmission standards
- Advanced neuroimaging to map brain changes
- Development of new drugs targeted
Current research offers real hope for millions of people affected by anorexia nervosa, promising more effective and personalised treatments in the near future.

Myths and Truths about Anorexia
| Myth | Truth |
| "Anorexia is vanity, or wanting attention" | Anorexia nervosa is a serious mental illness with a proven neurobiological basis. It is not a choice or a voluntary behaviour. |
| "It only affects teenage girls" | It affects people of all ages, genders and social classes. 10-15% of cases are men, and the condition can develop in childhood or adulthood. |
| "It's just a phase that passes by itself" | Anorexia nervosa rarely resolves without professional treatment. Without intervention, it has a mortality rate of 10-20%. |
| "You have to be very thin to have anorexia" | The DSM-5 removed specific weight criteria. People of "normal" weight can have equally severe atypical anorexia nervosa. |
| "It's impossible to recover completely" | With proper treatment, around 50% people recover completely, and many others have significant improvement. |
| "Exercise is always harmful" | Moderate, supervised exercise can be part of recovery, but excessive exercise is always harmful. |
| "The family must force the person to eat" | Force-feeding can aggravate the condition. Support should be provided with specialised professional advice. |
Resources and support available in Portugal
Portugal has several resources and organisations dedicated to supporting people with anorexia.
| Resource | Description | Contact |
| National Health Service (SNS) | Child psychiatry, psychiatry and psychology consultations through the family doctor | Family doctor |
| SNS 24 line | 24-hour telephone support for health issues | 808 24 24 24 |
| University Hospitals | Specialist consultations on eating disorders | Several central hospitals |
| Specialised Inpatient Units | Intensive treatment for severe cases | Júlio de Matos Hospital, Santa Maria Hospital |
| Lisbon Psychiatric Hospital Centre | Outpatient clinic specialising in eating disorders | 213 828 100 |
| SPPSM - Portuguese Society of Psychiatry and Mental Health | Information, training and support for professionals and families | Contact through specialised hospitals |
| Life Helpline | Emotional support and suicide prevention | 213 544 545 |
| SOS Friendly Voice | Telephone support for crisis situations | 213 544 545 |
In NeuroPsyqueWe are part of a network of specialised care, offering a response that combines Neurology, Neuropsychology, Psychiatry, PNEI, e Neurotherapy.
Our commitment is, as always, to provide you with the greatest possible expectation of improvement.
We have the most specialised equipment and specialists in therapies such as Transcranial Magnetic Stimulation and Transcranial Electrical Stimulation, which have proved important in the treatment of anorexia. Book your appointment with us!
Conclusion
Anorexia nervosa is a complex and serious eating disorder that profoundly affects not only the person diagnosed, but also their entire family and social network. Although it is the psychiatric disorder with the highest mortality rate, it is essential to emphasise that there is real hope e effective treatments available.
Key points to remember:
Anorexia nervosa it's not a choice or a "phase" - is a serious medical condition with a neurobiological basis that requires specialised treatment. O early diagnosis and intervention are crucial for a favourable prognosis, with recovery rates of more than 80% in adolescents when treatment is started quickly.
O multidisciplinary treatmentThe new approach, combining medical, psychological, nutritional and neurotherapeutic approaches, offers the best hope of recovery. Recent genetic research confirms that anorexia nervosa has both psychiatric and metabolic components, paving the way for increasingly personalised and effective treatments.
To families and carersIt is essential to understand that recovery is a long process that requires patience, specialised support and understanding. Combating stigma and myths about anorexia nervosa is fundamental to facilitating access to appropriate treatment and support.
There is hope. Each person is unique, and finding the ideal therapeutic combination may take time and adjustments, but it's worth persevering.
In NeuroPsyqueWe work every day to give best possible expectation of improvement to our patients, using a truly integrated approach that combines the best of neurology, neuropsychology and advanced neurotherapy. Book an appointment with us and find out how we can help you regain a healthy relationship with food and your body!
Questions and answers about Anorexia
1. Can anorexia nervosa be cured?
Anorexia nervosa is not "curable" in the traditional sense (the complete and definitive elimination of the disease, with no possibility of it returning), but it is highly effective treatment. With appropriate specialised follow-up, around 50% people recover completely, 25% have significant improvement, and the remaining 25% can benefit from continued treatment. The prognosis is much better when treatment is started early.
2. What's the difference between anorexia nervosa and dieting?
Anorexia nervosa involves body image distortion (seeing yourself as "fat" when you're thin), intense fear from gaining weight, and compulsive behaviour that the person can't control. A normal diet is flexible e does not compromise health or social functioning. Anorexia seriously interferes with everyday life.
3. How is anorexia nervosa diagnosed?
The diagnosis is clinicalbased on the DSM-5 criteriaIt includes a complete medical assessment: dietary restriction with low weight, intense fear of gaining weight, and distortion of body image. It includes a full medical assessment, physical examination, laboratory analyses and psychological assessment. There is no specific definitive test - the diagnosis must be made by specialised professionals.
4. Does anorexia nervosa only affect teenagers?
No. Although it is more common in adolescence (14-17 years), it can develop at any agefrom childhood to adulthood. Around 10-15% of cases occur in men, and the incidence in older people is increasing.
5. How long does the treatment take?
Treatment varies according to severity and individual response. A acute phase can last 6-12 months, but the full monitoring often lasts 2-5 years. A neurotherapy can speed up recovery, and early treatment significantly reduces the time required.
6. Is neurotherapy effective for anorexia nervosa?
Yes, very effective. Transcranial Magnetic Stimulation and Transcranial Electrical Stimulation (tDCS) have been shown to remarkable results in reducing symptoms and improving mood. These therapies are safe, without side effects and can be combined with other approaches.
7. How can the family help with recovery?
The family plays a role crucial to recovery. They can help through: emotional support without judgement, creating a calm environment during meals, avoiding comments about weight or food, looking for specialised family therapyand taking care of their own mental health. Informed family support significantly improves the prognosis.
8. What are the main warning signs?
Physical signs: Rapid weight loss, extreme fatigue, amenorrhoea, sensitivity to cold. Behavioural signs: Avoiding meals, obsessive calorie counting, excessive exercise, social isolation. Psychological signs: Obsessive preoccupation with weight, distortion of body image, extreme anxiety related to food.
9. Can anorexia nervosa cause death?
Unfortunately, yes. Anorexia nervosa has the higher mortality rate of all psychiatric disorders - approximately 10% per decade. The main causes are cardiovascular complications, electrolyte imbalances and suicide. This is why it is it's crucial to seek specialised treatment immediately.
10. Are there support groups in Portugal?
Yes, there are resources available through the NHS, specialised hospitals, and some support associations. Follow-up can include support groups for patients and families.
11. How do I explain anorexia nervosa to others?
It's important educate about the medical nature of the condition: explain that it is a severe mental illness neurobiological basis, not a choice. Emphasise that comments about weight or appearance can be harmful, and that the support without judgement is essential. Share reliable educational resources to help others understand the disease.
12. Does treatment always require hospitalisation?
Not all the time. The treatment outpatient clinic is often effective, especially when started early. O hospitalisation is necessary when there is a serious medical risk (very low BMI, heart problems, suicidal ideation) or when outpatient treatment is not working. A most patients can be treated on an outpatient basis (without hospitalisation) with regular specialised monitoring.




2 responses
I have a 15-year-old daughter with a diagnosis of purgative anorexia nervosa, and I would like indications of this transcranial stimulation treatment in Brazil (São Paul/SP).
Thank you for sharing this content, it was very enlightening.
Good morning, transcranial electrical and magnetic stimulation can be an effective therapeutic alternative for treating eating disorders.
There is a clinic in São Paulo:
https://reabilitarclinica.com/neuromodulacao/
This clinic could be interesting!
Thank you. If you come to Portugal, we have protocols to help.